What you’ll learn in this article…
- Introversion, shyness, and social anxiety require different strategies in clinicals.
- Working as a CNA or PCT builds bedside confidence through repeated exposure.
- Specialties like informatics and research match introverted working styles well.
A nursing student finishes first year with strong exam scores, completes two hospital rotations, and then starts a pulmonology externship only to discover that knowing every technique on paper does not stop the mind from going blank at a real patient's bedside. That is exactly what Reddit user faeleafs described in a 2026 post on r/Nurses: freezing mentally and physically during patient interactions, apologizing to patients who never asked for an apology, and crying over mistakes that any first-year student would make.1
The gap between academic performance and clinical confidence is one of the most common, least discussed struggles in nursing education. It cuts across ADN, BSN, and graduate-level programs alike. Introverted and highly empathetic students are especially vulnerable, not because they lack competence, but because the leap from controlled exam conditions to unpredictable bedside encounters demands a skill set that textbooks alone cannot build.
Introversion Vs. Shyness Vs. Social Anxiety: What's Actually Going On
Feeling energized after hours alone with your pathophysiology textbook versus feeling paralyzed when introducing yourself to a patient are two completely different phenomena, yet nursing students often conflate them. Understanding the distinction between introversion, shyness, and clinical social anxiety is the first step toward building a sustainable clinical practice.
Introversion Is About Energy, Not Ability
Introversion describes where you recharge, not whether you can function in social or clinical settings. Personality psychology research, including foundational work by psychologist Hans Eysenck and later refinements by Susan Cain, frames introversion as a preference for lower-stimulation environments. Introverts process social interaction differently, often requiring solitude to restore mental energy after prolonged patient contact, team meetings, or simulation labs. This preference has zero correlation with clinical competence, communication skill, or bedside effectiveness. Many accomplished nurses, nurse practitioners, and clinical educators identify as introverts and simply build recovery time into their routines.
Shyness and Social Anxiety Occupy a Different Spectrum
Shyness involves temporary discomfort or self-consciousness in unfamiliar social situations. It typically diminishes with repeated exposure and can be managed through deliberate practice, cognitive reframing, and structured skill-building. Social anxiety disorder, by contrast, is a persistent, intense fear of scrutiny or judgment that significantly impairs functioning. When a student avoids clinical rotations, cries after minor instructor feedback, or apologizes compulsively to patients (even when no error occurred), the pattern may sit at the shyness-anxiety boundary and warrant professional assessment.
Self-Assessment Helps You Choose the Right Strategy
If you freeze mentally and physically despite acing exams, ask yourself: Do I feel drained after clinicals but capable during them (introversion)? Do I feel nervous but improve with practice (shyness)? Or do I avoid patient contact, ruminate over small corrections for days, and experience physical symptoms like sweating or nausea before shifts (possible social anxiety)? Each category responds to different interventions. Introverts benefit from planned downtime and low-stimulation study spaces. Shy students improve with incremental exposure, role-play, and pre-shift mental rehearsal. Students experiencing clinical anxiety may need cognitive-behavioral strategies, campus counseling, or formal accommodations. tips to deal with anxiety for the nervous new nurse can offer practical starting points for those uncertain where their experience falls on this spectrum.
Recognition Unlocks the Right Tools
Many successful nurses are introverts. Recognizing where you fall on this spectrum allows you to select coping mechanisms that fit your actual challenge rather than forcing yourself into a mold designed for extroverts. The goal is not to become someone else but to build skills and structures that let your natural strengths emerge in patient care.
Why Introverts Actually Make Excellent Nurses
Introverts possess clinical strengths that nursing programs increasingly recognize as essential to patient safety and quality care. Far from being a liability, the introspective tendencies that make bedside interactions feel exhausting are often the same qualities that prevent errors and build deeper patient trust.
The Research on Introvert Performance
Nursing education research reveals a more nuanced picture than the stereotype of the outgoing nurse might suggest. Studies examining personality preferences among nursing students have found that common personality types in nursing programs include both extroverted types (ENFP) and introverted types (ISTJ, ISFJ), indicating that the profession attracts and retains both temperaments successfully.1
Research published through the Biomedical Research Network found statistically significant relationships between learning styles and caring behaviors among nursing students, with extraversion and introversion showing a meaningful connection to how students demonstrate care (p < 0.001).1 That finding suggests introverts may simply express caring differently rather than less effectively. Similarly, studies on personality preferences and stress perception among nursing students have identified significant differences in how introverts and extroverts experience clinical stress (p < 0.001), though both groups can develop effective coping mechanisms.2
Strengths That Translate to Safer Practice
Introverts bring specific cognitive tendencies that align remarkably well with nursing competencies:
- Deep listening: Introverts naturally focus on what patients say rather than formulating their next response, catching subtle symptoms or concerns that rapid conversationalists might miss.
- Careful observation: The tendency to watch before acting means introverts often notice changes in patient condition, nonverbal cues, or environmental hazards earlier.
- Thorough documentation: A preference for written over verbal communication translates to more complete, accurate charting.
- Reflective decision-making: Thinking before acting reduces impulsive errors and promotes evidence-based practice.
Reframing the Core Fear
If you are asking yourself whether you are fit for nursing because patient interactions drain you, consider this reframe: the mental energy you expend during each interaction reflects how seriously you take it. That conscientiousness protects patients.
As one experienced nurse noted in discussing common nursing school anxieties, serious errors like administering NG tube formula into an IV line come from carelessness and rushing, not from being quiet or reserved.3 The introvert's natural caution serves as a built-in safety mechanism. Your tendency to double-check, to pause before acting, and to replay interactions in your mind afterward are not weaknesses to overcome. They are clinical assets that many extroverted colleagues must consciously develop. The question is not whether introverts can succeed in nursing but how to leverage these strengths while building sustainable energy management strategies.
Questions to Ask Yourself
How Instructors and Preceptors Evaluate Communication in Clinicals
Domain 9 of the 2021 AACN Essentials establishes communication as a core competency for all nursing graduates, breaking it into three subdomains: Therapeutic Communication, Professional Boundaries, and Professional Communication.1 Understanding exactly what your clinical instructors measure removes the guesswork that often amplifies anxiety for quieter students.
What Clinical Rubrics Actually Assess
Clinical evaluation tools vary by program, but they share common threads. The Washington State University BSN Clinical Evaluation Tool, for example, requires students to demonstrate communication through specific frameworks: AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You), ISBAR/SBAR for handoffs, and active listening during patient interactions.2 Written communication standards also appear, including correct spelling, grammar, and sentence structure in documentation.2
Appalachian State University's BSN Pre-Licensure Progression Tool breaks therapeutic communication into observable behaviors: eye contact, active listening, appropriate touch, and appropriate questions.3 Notice that none of these require you to be outgoing or talkative. They require presence, attentiveness, and purposeful engagement.
Mohave Community College's ADN Clinical Evaluation Tool measures seven competencies,4 while Montana State University uses a checklist format with a dedicated "Communication" section.5 The OB Clinical Evaluation Tool referenced in nursing education literature uses a five-factor scoring system where a score of 2 indicates satisfactory performance with only occasional guidance needed, while a score of 1 (unsatisfactory) reflects persistent need for guidance.6 The distinction centers on independence and consistency, not personality.
What "Good Enough" Communication Looks Like
Instructors are not searching for extroverted charisma. They evaluate safety, clarity, and patient-centered engagement. A student who speaks quietly but delivers accurate information using SBAR format meets the standard. A student who pauses to gather thoughts before responding demonstrates thoughtfulness, not weakness. Research on nursing simulation labs and nursing education reinforces this point: structured practice builds competence without requiring a personality overhaul.
Satisfactory communication means you initiate patient interactions without excessive prompting, use therapeutic techniques like open-ended questions and reflective statements, collaborate with the healthcare team, and assert yourself when patient safety requires it.7 You do not need to fill every silence or project an energetic demeanor.
Professional Behavior Carries Significant Weight
Many rubrics weigh professional behaviors alongside verbal communication skills. Punctuality, preparation, willingness to ask questions, and receptiveness to feedback often account for substantial portions of clinical evaluations. Shy students who arrive early, review patient charts thoroughly, and come prepared with questions already demonstrate professionalism that instructors document favorably.
The Washington State University tool requires completion of at least five shift reports, emphasizing documentation and handoff communication over spontaneous social interaction.2 If you prepare your reports carefully and communicate essential information during handoffs, you fulfill a major rubric requirement regardless of how naturally conversation flows for you.
Reframe the Rubric as Your Roadmap
Ambiguity fuels anxiety. When you do not know what is being measured, you default to vague goals like "be more outgoing" or "talk more." These targets feel impossible and unmeasurable.
Instead, obtain your program's clinical evaluation tool and study the specific criteria. If the rubric lists active listening, practice reflecting back what patients say. If it mentions SBAR, rehearse structured handoffs until they feel automatic. If professional boundaries appear, review scenarios that test appropriate self-disclosure.
When you know exactly what behaviors earn a satisfactory score, you can target those behaviors directly. You stop trying to change your personality and start building specific, observable skills. This shift transforms clinical preparation from an exercise in self-criticism into a practical checklist you can actually complete.
A Step-By-Step Confidence-Building Plan for Clinical Rotations
Building clinical confidence is not a personality transplant. It is a skill, and like any skill in nursing, it improves with deliberate practice and repetition. The students who freeze at the bedside despite acing exams are not lacking intelligence or compassion. They are lacking exposure. The solution is a structured progression that gradually increases the stakes while your competence catches up to your knowledge.
Week-by-Week Exposure Hierarchy
A typical clinical rotation runs 8 to 12 weeks. Use the first third for observation and co-performance, the middle third for supervised independence, and the final third for autonomous practice with debrief.
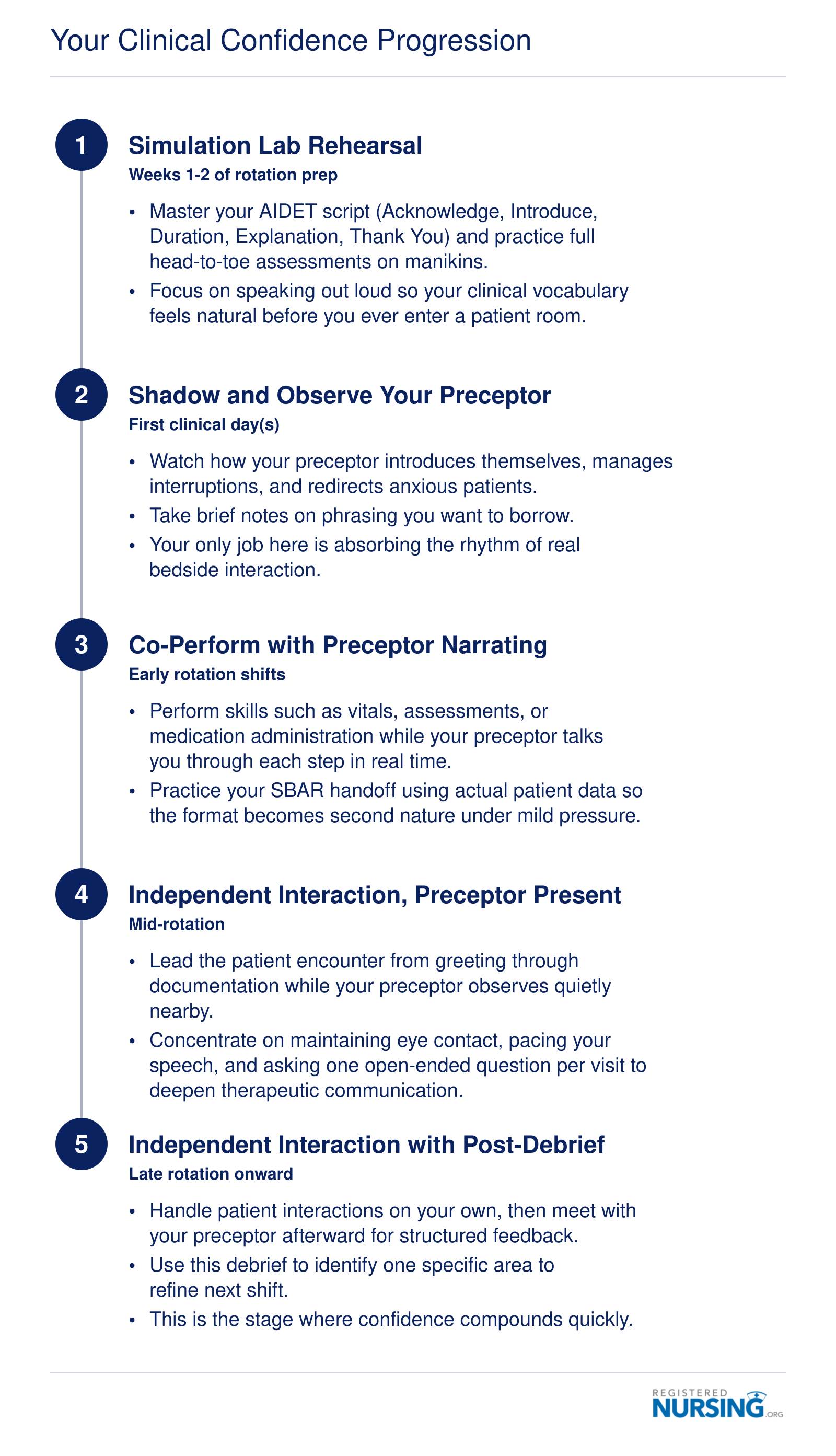
- Weeks 1-2: Simulation lab and observation. Practice your introduction, vital signs, and head-to-toe assessment on mannequins and peers. Shadow your preceptor during patient interactions without speaking. Your only job is to watch how they phrase questions, handle awkward silences, and transition between tasks.
- Weeks 3-5: Co-performance. Your preceptor introduces you, and you perform one discrete task per patient visit (e.g., blood pressure check, wound dressing). Debrief immediately afterward. Ask what you did well before asking what to improve.
- Weeks 6-8: Lead with backup. You knock, introduce yourself, and complete the full interaction while your preceptor observes from the doorway or bedside. They intervene only if you miss something critical.
- Weeks 9-12: Independent with debrief. You take the assignment, perform care, and report back. Your preceptor spot-checks your documentation and listens to your SBAR handoff.
This hierarchy mirrors the advice shared by Either_Jello7730, a nurse who described the value of repetitive, low-stakes exposure. They recommended taking a CNA or PCT job specifically for this reason: volume of patient interactions desensitizes the fear response. If you perform ten bed baths in a shift, the eleventh stops feeling like a performance.
Communication Scripts You Can Memorize
Anxiety disrupts working memory. When your mind goes blank, a pre-memorized script is your safety net. Two frameworks cover most student clinical communication.
AIDET for patient introductions:
- Acknowledge: "Good morning, Mr. Smith. I see you've been waiting for pain medication."
- Introduce: "My name is [Your Name], I'm a nursing student working with Nurse [Preceptor Name] today."
- Duration: "I'll be with you for about five minutes to check your vitals and your IV site."
- Explanation: "I'm going to take your blood pressure, temperature, and oxygen level, then I'll look at your IV to make sure it's comfortable."
- Thank You: "Thank you for letting me practice. I'll let Nurse [Preceptor] know you're ready for that pain med."
SBAR for nurse-to-provider handoff:
- Situation: "This is [Your Name], student nurse on 4 West. I'm calling about Mr. Smith in room 412, who has increased shortness of breath."
- Background: "He's post-op day two from a knee replacement, no prior respiratory history. Vital signs at 0800 were stable."
- Assessment: "Current oxygen saturation is 88% on room air, respiratory rate 28, he's using accessory muscles."
- Recommendation: "I think he needs a chest X-ray and supplemental oxygen. Can you come evaluate him?"
The Simulation-to-Bedside Bridge
The night before clinicals, rehearse the exact scenario you will face. If you know you will be doing a Foley catheter insertion tomorrow, run through the procedure in the simulation lab or with a peer tonight. Speak the words out loud: "I'm going to clean the area now. You might feel some pressure." When the moment arrives at the bedside, your procedural memory takes over and the anxiety has less room to hijack your performance.
This is not about being fake or scripted. It is about ensuring that when your sympathetic nervous system floods your prefrontal cortex, the words are already there.
Your Clinical Confidence Progression
Building clinical confidence is not a switch you flip. It is a graduated exposure process, moving from controlled practice to independent patient care. Each step layers new skills onto the last, so you grow steadily rather than being thrown into the deep end.
Real Talk: When Academic Success Doesn't Match Clinical Confidence
Acing exams does not predict bedside confidence, and the gap between the two is not a character flaw. It is a predictable, well-documented phenomenon in nursing education. A student can finish first year with strong grades, complete two hospital rotations, land a competitive pulmonology externship, and still freeze the moment a real patient makes eye contact. That is the exact situation one nursing student described publicly on r/Nurses in 2026,1 and the responses from working nurses were unanimous: this is normal, and it passes with exposure.
Why Your Brain Treats Testing and Clinicals as Different Tasks
Exam performance draws on recall inside a quiet, controlled environment where the only variable is you and the question. Clinical work layers on sensory overload (alarms, smells, unfamiliar equipment), time pressure, and continuous social evaluation from patients, families, preceptors, and staff. Your nervous system reads those inputs as threat cues and shunts blood away from the prefrontal cortex, the exact region you need for clinical reasoning. So you go blank, not because you don't know the material, but because your brain has temporarily prioritized survival over recall. Repeated, low-stakes exposure is what retrains that response. There is no shortcut around the reps.
Three Bridges From Knowing to Doing
- Pre-shift mental rehearsal: Before clinical, spend ten minutes walking through likely scenarios for your assigned unit. Picture the room entry, the introduction, the assessment sequence, the questions a patient might ask. Athletes call this visualization; it measurably reduces performance anxiety.
- A pocket script card: Write out SBAR handoff structure and AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You) on an index card. When your mind blanks, you read. Nobody will judge you for glancing at a card in your first year.
- CNA or PCT work between semesters: High-volume, low-complexity patient contact (bathing, vitals, ambulation, feeding) builds procedural comfort with touch, positioning, and conversation. Multiple commenters on that Reddit thread named this as the single biggest confidence builder they experienced.1
The Timeline Nobody Tells You
Most nursing students do not feel clinically confident until deep into their second year, and many describe the real shift happening three to six months into their first RN job. Nursing simulation labs offer one structured way to close that gap before graduation. Feeling shaky during a first year externship is developmentally on track, not a warning sign. The students who quit tend to be the ones who assumed everyone else felt ready. They didn't.
Related Articles
Managing Excessive Apologizing, Crying, and Emotional Overwhelm
You can either swallow your emotions until they overflow in the middle of a patient interaction, or you can learn to name, accept, and channel them before they take over. The first path feels safer in the short term but often backfires; the second takes practice but builds genuine clinical confidence.
The Apology Habit: Recognizing When "I'm Sorry" Isn't Helping
Apologizing for minor things, like fumbling with equipment or asking a clarifying question, can make you seem less competent to patients and preceptors. It also reinforces your own inner narrative that you are a problem. Instead of saying "I'm sorry" for needing another set of hands, try "Thank you for your patience" or "I appreciate your guidance." This swaps a self-diminishing statement for one that acknowledges the team's support while keeping your professional presence intact.
Handling Tears on the Clinical Floor
Crying is a physiological release, and in a high-stakes environment like a hospital, it is understandable. But when tears come at the bedside, patients may feel unsettled. If you feel the wave rising, give yourself a brief script: "I need to check on a supply for a moment." Step into a break room or restroom, let the release happen, and then splash cold water. Composing yourself with a few deep breaths can reset your nervous system. Over time, you will build tolerance, and the triggers will lose some of their power.
Desensitization Through Gradual Exposure
Research on performance anxiety points to progressive exposure as one of the most reliable strategies. Start with the least threatening patient interactions, perhaps taking vitals for a stable patient while a preceptor stands nearby. As those become routine, add a brief conversation, then a more complex procedure. Simulation labs are an ideal space for this: many programs now incorporate scenarios specifically designed to evoke mild stress, so you can practice emotional regulation without real-world consequences. The goal is not to eliminate anxiety but to function effectively alongside it.
Mindfulness and Self-Talk That Actually Work
In the moment, grounding techniques can interrupt panic: notice five things you can see, four you can touch, three you can hear. Before a clinical day, set an intention: "I will notice when I feel overwhelmed and take a slow breath before acting." Cognitive reframing also matters. When you catch yourself thinking, "I'm going to mess up," counter with, "I have prepared for this, and my instructors believe I can do it." Over weeks, these mental habits build the confidence that exams alone cannot provide. Self-care for nurses is a practical place to start, and many nursing organizations and campus counseling services also offer workshops on stress resilience, making them a worthwhile step toward steady emotional control.
Try this swap: instead of "I'm sorry, I need to check that," say "Great question, let me confirm the most current information for you." Same empathy, more authority. Rehearse the phrase three times aloud in sim lab before your next clinical day so it feels natural at the bedside.
Nursing Specialties and Career Paths That Suit Introverts
The real tension here is not whether introverts belong in nursing. It is whether every nursing role demands the same kind of social energy, and the answer is no. Choosing a specialty that matches your natural working style is not a workaround or a concession. It is smart career planning.
One important clarification before the list: introvert-friendly does not mean patient-free. Nearly every nursing role involves human connection. What varies is the volume, predictability, and depth of those interactions. Introverts typically do their best work in environments where conversations are purposeful and one-on-one rather than constant and high-volume. Many specialties offer exactly that.
Specialties With Very Low Daily Patient Interaction
- Nursing Informatics: Work centers on data systems, electronic health records, and workflow analysis. Patient contact is essentially absent from day-to-day duties. Deep analytical focus and structured project meetings are the primary demands, making this one of the strongest fits for introverts who want to apply clinical knowledge in a behind-the-scenes role.1
- Infection Control: Infection preventionists spend most of their time reviewing surveillance data, identifying patterns, and developing protocols. Direct patient contact is rare. The work rewards systems thinking and careful documentation, with interactions that tend to be consultative and scheduled rather than spontaneous.
Specialties With Structured or Episodic Interaction
- OR/Perioperative Nursing: Patient contact exists but is brief. Pre-op assessment and post-op check-ins are focused and time-limited. The bulk of the workday involves a skilled, stable team operating in a quiet, procedure-driven environment with very little casual socializing.2
- Radiology and Interventional Radiology Nursing: Interactions are almost entirely one-on-one and procedure-specific. The physical environment tends to be calm, and patient volume is manageable. Focused attention and the ability to put anxious patients at ease in a short window are genuine strengths here.2
- Forensic Nursing: Work is procedural and documentation-intensive. Whether conducting sexual assault examinations or working within a legal-medical interface, the role demands precision and careful attention to detail. Interactions are structured by protocol, which suits nurses who prefer clear frameworks.4
- Research Nursing: Patient interaction is moderate but purposeful. Conversations follow a protocol script, and a significant portion of the role involves solo data management and regulatory documentation. The work rewards sustained focus over a long arc rather than rapid-fire multitasking.1
- Case Management: Coordination happens in episodes rather than continuously. Case managers typically communicate with patients and families around specific goals and transitions, with meaningful autonomy over their schedule and workflow.1
Advanced Practice Paths Worth Considering
- Psychiatric-Mental Health Nurse Practitioner (PMHNP): At first glance, a full day of appointments sounds demanding for an introvert. In practice, the PMHNP role is built on deep listening and one-on-one therapeutic relationships, which many introverts find energizing rather than draining. Conversations are meaningful and unhurried, and the reflective nature of psychiatric work aligns well with introverted processing styles. The advanced practice pathway requires a graduate degree at the master's or doctoral level and national certification as a PMHNP.4
If you are weighing which graduate-level direction fits your strengths, reviewing career paths for advancing nurses can help you map the options before committing to a program. No specialty guarantees a stress-free experience, and every role will ask you to stretch occasionally. What this list offers is a realistic map of where your natural tendencies, including focused attention, careful observation, and comfort with depth over breadth, become professional assets rather than things to overcome. For introverts who want to step further back from the bedside, nursing jobs that let you work from home represent another growing category worth exploring.
When to Seek Help: Accommodations, Counseling, and Support Resources
The Americans with Disabilities Act, along with Section 504 of the Rehabilitation Act, requires accredited nursing programs to provide reasonable accommodations to students with documented anxiety disorders. That legal foundation matters, because too many nursing students suffer through preventable distress simply because they do not know support is available or feel too ashamed to ask.
Knowing When Discomfort Becomes Impairment
Feeling nervous before a clinical shift is normal. Introversion is not a disorder, and even shyness fades with practice for most students. The line that separates ordinary social discomfort from something that warrants professional attention is functional impairment. Ask yourself whether anxiety is causing you to avoid clinical rotations, leave required patient interactions incomplete, or experience physical symptoms like nausea, chest tightness, or full panic attacks. If the answer is yes, that is not a personality quirk to push through alone. That is a clinical picture worth discussing with a licensed mental health provider.
How to Request Accommodations
The process is more straightforward than most students expect:
- Start with disability services: Every accredited school has an office. Register there first, before approaching the nursing department directly.
- Bring documentation: A letter or evaluation from a licensed psychologist, psychiatrist, or licensed clinical social worker describing your diagnosis and functional limitations is typically required.
- Collaborate on reasonable supports: Once registered, you and the disability office work together to identify accommodations the nursing program can realistically provide. Common examples include placement in smaller clinical groups, additional simulation lab time to rehearse patient interactions, and modified oral presentation formats.
Accommodations are negotiated, not guaranteed in any specific form, so being clear about which situations trigger the most impairment helps the process move efficiently.
Support Resources Worth Knowing
Campus counseling centers are an underused asset. Most offer free short-term therapy, and many use cognitive behavioral therapy, which has a strong evidence base for social anxiety. If your campus waitlist is long, the NAMI HelpLine (1-800-950-NAMI) connects callers to trained volunteers who can help identify local resources. The Anxiety and Depression Association of America maintains a therapist directory at adaa.org, organized by specialty and location.
Nursing student peer mentorship programs, where they exist, pair newer students with upperclassmen who have navigated similar challenges. Ask your program coordinator whether one is available.
Addressing the Stigma Directly
Requesting accommodations is not cheating, and it carries no professional penalty. Disability records are kept confidential under FERPA and the ADA. They are not shared with the nursing board during licensure and will not appear anywhere on your RN licensing timeline. Schools are legally prohibited from disclosing that information. Seeking support is an act of self-awareness, the same quality that makes nurses good at advocating for their patients.
Common Questions About Being an Introverted Nursing Student
These are the questions we hear most often from nursing students who identify as introverted, shy, or socially anxious. Each answer points you to a deeper discussion elsewhere in this guide.
- Can I be a nurse if I'm shy?
- Absolutely. Shyness is not a disqualifier. Many nurses describe themselves as shy early in training yet go on to build strong therapeutic relationships with patients. The key is learning to separate personal discomfort from professional communication, a skill that improves with structured practice. See the section on why introverts actually make excellent nurses for a closer look at the strengths you already bring to the bedside.
- How do I overcome shyness in nursing school clinicals?
- Start with small, repeatable wins. Introduce yourself to every patient using a scripted opening, then gradually layer in assessment questions as your comfort grows. As one commenter on Reddit's r/Nurses shared, working as a PCT or CNA outside of school hours provides extra exposure that accelerates confidence. Our step-by-step confidence-building plan for clinical rotations breaks this progression down week by week.
- What nursing specialties are best for introverts?
- Specialties with more structured or one-on-one patient interactions tend to suit introverts well. Informatics, research nursing, perioperative nursing, public health, and certain telehealth roles offer environments where deep focus and careful analysis are prized over rapid-fire social interaction. The section on nursing specialties and career paths that suit introverts explores these options in detail.
- Is social anxiety a barrier to becoming a nurse?
- Social anxiety can make clinical rotations more challenging, but it does not have to stop you. Many students freeze or over-apologize during patient encounters, as one nursing student recently described in a Reddit post about starting a pulmonology externship. With targeted strategies and, when needed, professional counseling, social anxiety is manageable. Our section on when to seek help covers accommodations and campus resources.
- How do nursing instructors evaluate communication skills in clinicals?
- Instructors typically assess therapeutic communication: how you introduce yourself, explain procedures, ask open-ended questions, and respond to patient concerns. They are looking for professionalism and patient-centered dialogue, not extroversion. Quiet students who listen attentively and document thoroughly often score well. The section on how instructors and preceptors evaluate communication explains what rubrics usually prioritize.
- What is the difference between introversion and social anxiety in nursing?
- Introversion is a personality trait; you recharge through solitude but can interact effectively when needed. Social anxiety is a clinical condition that triggers intense fear, mental freezing, or physical symptoms during interactions. One does not automatically lead to the other, but they can overlap. Our earlier section on introversion vs. shyness vs. social anxiety helps you identify where you fall and what support may help.
- Can I get accommodations for social anxiety in nursing school?
- Yes, if social anxiety is documented by a licensed provider, most nursing programs offer accommodations through their disability services office. These may include extra time in simulation debriefs, modified group presentation formats, or access to counseling. Accommodations do not lower academic standards; they level the playing field. The section on accommodations, counseling, and support resources walks you through how to initiate that conversation.
The student who freezes at the bedside today is building the exact neural pathways that will make them a vigilant, detail-oriented nurse tomorrow. The discomfort is temporary; the strengths are permanent. If you see yourself in the story of a nursing student who aces every exam yet apologizes to patients for breathing, take three concrete steps. Use structured communication frameworks like SBAR and AIDET so your words have a reliable scaffold even when your nerves spike. Pursue high-volume, low-stakes patient exposure through CNA or PCT work to build the muscle memory that lectures alone cannot provide. And if anxiety crosses from uncomfortable into functionally impairing, seek support early through your program's counseling services or disability office before small struggles calcify into larger ones.
Nursing needs more careful listeners, deep thinkers, and empathetic observers. It needs introverts. Your quiet presence is not a deficit to overcome. It is exactly what your future patients deserve.