Standard Precautions, Transmission Based, Surgical Asepsis: NCLEX-RN
- Understanding Infections and Communicable Diseases and the Modes of Organism Transmission
- Applying the Principles of Infection Control
- Using Appropriate Technique to Set up a Sterile Field and Maintaining Asepsis
- Following the Correct Policy and Procedures When Reporting a Client With a Communicable Disease
- Educating the Client and Staff Regarding Infection and Infection Control Measures
- Utilizing Appropriate Precautions for Immunocompromised Clients
- Evaluating Infection Control Precautions That Are Implemented by Staff Members
- Evaluating Whether Aseptic Technique is Performed Correctly
In this section of the NCLEX-RN examination, you will be expected to demonstrate your knowledge and skills standard precautions, transmission-based, and surgical asepsis in order to:
- Assess client care area for sources of infection
- Understand communicable diseases and the modes of organism transmission (e.g., airborne, droplet, contact)
- Apply principles of infection control (e.g., hand hygiene, surgical asepsis, isolation, sterile technique, universal/standard precautions)
- Use an appropriate technique to set up a sterile field/maintain asepsis (e.g., gloves, mask, sterile supplies)
- Follow correct policy and procedures when reporting a client with a communicable disease
- Educate client and staff regarding infection control measures
- Utilize appropriate precautions for immunocompromised clients
- Evaluate infection control precautions implemented by staff members
- Evaluate whether the aseptic technique is performed correctly
Some of the commonly used terms and terminology associated with infection control include those relating to the chain of infection, the modes of transmission of infectious microorganisms, asepsis, types of infection, and personal protective equipment. Read more about cleaning, disinfection, and sterilization.
- The chain of infection includes the infectious microorganism, the reservoir or location where the pathogen lives, the port of exit from the reservoir, the mode of transmission from the reservoir, the portal of entry into the person, or host.
- Airborne transmission is defined as the mode or means with which a microorganism is moved and transmitted via air and inhaled into the respiratory tract by the susceptible host. These infections are found in droplets and dust in the air. Airborne precautions are indicated in the presence of a pathogen that is transmitted via the airborne mode of transmission.
- Contact transmission is defined as the mode or means with which a microorganism is moved and transmitted via direct or indirect contact with the infected person or an object that has been contaminated with the pathogen, respectively. Indirect contact transmission is sometimes referred to as vehicle-borne transmission. Contact precautions are indicated in the presence of a pathogen that is transmitted via contact transmission.
- Vector-borne transmission is defined as the transmission of a pathogen from an animal or insect to a human being.
- Transmission based precautions are special measures that are put in place to prevent the spread of infection. Transmission based precautions are based on the pathogens mode of transmission. Examples include contact and airborne precautions.
- Standard precautions are measures that are used to prevent the spread of infection among all patients whether or not they have a known infection. Standard precautions protect health care workers and patients from the spread of infection secondary to contaminated blood and other bodily fluids.
- Asepsis is defined as not septic, that is, asepsis is the absence of disease-causing organisms. The two types of asepsis are medical asepsis and surgical asepsis.
- Medical asepsis is defined as the absence of disease-causing microorganisms. Medical asepsis is often referred to as clean which is more than sanitary. Medically aseptic techniques are used to maintain medical asepsis.
- Surgical asepsis is defined as the absence of all microorganisms. Surgical asepsis is often referred to as sterile. Surgically aseptic techniques are used to maintain sterile asepsis.
- Contaminated is defined as some contact with a microorganism. Sterile items and clean or medically aseptic items are contaminated differently. A medically aseptic item is contaminated with it comes in contact with pathogenic microorganisms and sterile items become infected when they are touched with any item that is not sterile.
- Decontamination, according to OSHA, is defined as “the use of physical or chemical means to remove, inactivate, or destroy bloodborne pathogens on a surface or item to the point where they are no longer capable of transmitting infectious particles and the surface or item is rendered safe for handling, use, or disposal.”
- Disinfection is defined as the destruction of pathogens, but not spores, using a chemical or physical means of disinfection.
- Sterilization is defined as the process with which all pathogens including spores are destroyed. Sterilization can be done with moist heat, a combination of heat and pressure, gas, radiation, and boiling water.
- An antiseptic is a germicidal solution that inhibits the growth of some microorganisms. Examples of antiseptics include hexachlorophene, iodine, alcohol, and antiseptic hand washes. Many can be used directly on the skin.
- Healthcare-associated infection is any infection that occurs during the time that the patient is being cared for in a health care facility. Most of these infections are infections of the urinary tract.
- Iatrogenic infections are those that occur as the result of some diagnostic test or therapeutic procedure. For example, atelectasis after a diagnostic bronchoscopy is an iatrogenic infection.
- Occupational exposure is an exposure to a pathogen by a health care worker during their course of work.
- Post-exposure prophylaxis is the prevention of an infection after an individual has been exposed to it.
- Personal protective equipment (PPE) is specialized equipment and attire that is used by employees in health care to protect against infections. Examples of personal protective equipment include gowns, gloves, masks, goggles, and respirators.
Assessing the Client Care Area for Sources of Infection
Throughout the delivery of patient care, nurses must constantly and continuously monitor and surveil the patent care environment for possible and likely sources of infection. Like all other safety concerns, nurses must report and correct all sources of infection in the patient care area. Health care-acquired infections are costly and highly concerning events.
Technically speaking, healthcare-acquired infections are those infections that were contracted after the first health care contact or admission. Health care-acquired infections, sadly, are primarily passed along with the hands of the health care provider, therefore, proper handwashing is one of the primary things that the entire health care team can do to prevent them.
Some of the risk factors that impact on the frequency and occurrence of healthcare-acquired infections include immunosuppression, the close living quarters that clients and residents share, the prolonged state of illness that many patients have, surgeries, and some of the treatments that clients get such as the placement of an indwelling urinary catheter, chemotherapy, or the placement of an intubation tube.
The most commonly occurring pathogenic microorganisms that lead to healthcare-acquired infections are E.coli, staphylococcus aureus, pseudomonas aeruginosa, candida albicans, and enterococcus. The primary locations of these healthcare-acquired infections are surgical wounds, the urinary tract, the respiratory tract, and the bloodstream.
Understanding Infections and Communicable Diseases and the Modes of Organism Transmission
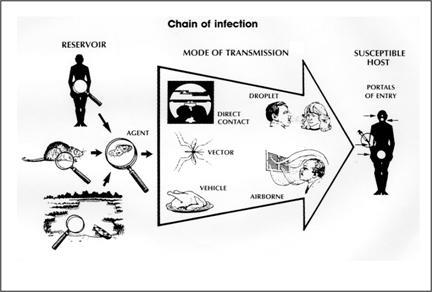
Source: Centers for Disease Control and Prevention. Principles of epidemiology, 2nd ed. Atlanta: U.S. Department of Health and Human Services; 1992.
The chain of infection includes:
- The pathogenic infectious microorganism
- The mode of transmission
- The reservoir
- The portal of exit
- The susceptible host
- The portal of entry
Communicable diseases and infections occur as the result of many pathogenic disease-causing fungi, bacteria, viruses, parasites, and prions. Prions are protein particles without nucleic acid that can cause neurological diseases like Creutzfeldt-Jakob disease and scrapie.
The Infectious Agent
Bacteria
Bacteria differ in terms of their morphology or shape, their actions, and their reactions to some laboratory diagnostic tests. Bacteria can be shaped like a rod, a circular cell, a sphere, or a spiral; some pathogenic bacteria lead to infection by releasing toxins into human tissue and some are gram-positive and others are gram-negative when they are tested in the laboratory, for example.
Rod-shaped bacteria are referred to as bacilli; round-shaped bacteria are referred to as cocci, and spiral-shaped bacteria are referred to as spirochetes. An example of bacillus is Bacillus anthracis which causes anthrax. Bacilli are gram-positive aerobic microorganisms. Examples of a coccus are staphylococcus and streptococcus, and examples of spirochetes are those that cause syphilis and Lyme disease.
Different bacteria react differently to diagnostic laboratory testing. Some bacteria are gram-positive and others are gram-negative, and some are characterized by their ability to change color, and others are characterized as resistant to color changes.
Gram-positive bacteria react to the introduction of a gram stain because they, anatomically, have a thick wall which contains peptidoglycan and teichoic acid; gram-negative bacteria do not react to a gram stain because these bacteria have thin walls that are comprised of a lipid membrane holding endotoxins such as lipoproteins and lipopolysaccharides. Gram-negative bacteria are more common than gram-positive bacteria.
Bacteria are also differentiated by their ability to resist color changes when subjected to a staining procedure in the laboratory. Acid-fast bacteria resist decolorization when stained with a Ziehl-Neelsen or Kinyoun stain.
The four phases of bacterial growth in the correct sequential order are:
- The lag phase: The lag phase is characterized by the bacteria's acclimation and adaptation to their environment; the bacteria mature but they are not ready for division and growth. RNA synthesis occurs, and the rate of biosynthesis is high because the bacteria need these proteins for the future, rapid growth.
- The log phase: The log phase, often referred to as the exponential phase and the logarithmic phase of growth is characterized by the bacteria's rapid and continuous growth until the nutrients, necessary for growth, no longer exist.
- The stationary phase: The stationary phase, which results from the depletion of the nutrients that are necessary for the continued growth of the bacteria, is characterized by the cessation of growth and the bacteria's metabolic activity.
- The death phase: The death phase is the end of the bacteria's life.
Viruses
Viruses are comprised of RNA, DNA, and long molecules; and they have an outer coat of protein that consists of lipids. They are also smaller than bacteria. Some viruses have a wide host range and others have a narrow and low host range. Viruses with a wide host range can infect and impact on multiple species, including human beings, and others with a narrow and low host range can impact on and infect as few as one species.
Viruses, like bacteria, come in several shapes including icosahedral and helical shapes, and they can be differentiated from each other in terms of their specific host cells. For example, some viruses are plant viruses and others can be categorized as fungal viruses or animal viruses. Lastly, they can also be according to their method of replication and their nucleic acid composition in terms of RNA and DNA.
The six stages of virus growth in correct sequential order are attachment, penetration, uncoating, replication, self-assembly, and release.
- The attachment stage: This stage is characterized by the virus attaching to a receptor on the host's cells. Some viruses are highly limited in terms of their ability to attach to host cells and others have a great ability to attach to host cells.
- The penetration stage: The penetration stage occurs with viral entry when the virus enters the host's cell.
- The uncoating stage: This stage entails the removal and destruction of the virus' coating; this action allows the virus to deposit its nucleic material into the host cell.
- The replication stage: The replication stage is characterized by the replication and multiplication of the virus.
- The self-assembly stage: The self-assembly stage is the stage with which the virus mature.
- The release stage: During the release stage the virus is released from the host cells and the virus dies as the result of its lysis.
RELATED: How Do Nurses Protect Themselves from Highly Infectious Patients?
Fungi
Fungi are found in the soil, on plant life, and on human beings. Most are harmless; however, there are some that can lead to serious infections among humans, particularly when the client is immunocompromised for one reason or another.
Fungi have what is referred to as a mutualistic symbiotic relationship, an antagonistic relationship, and a commensal symbiotic relationship with humans and also other organisms. These relationships with other organisms benefit both the host and the fungus, causing harm to the host of the fungus, and neither benefit or harm the host and fungus, respectively.
Humans, including our clients in the health care environment, can get superficial, cutaneous, subcutaneous, and systemic fungal infections. Systemic fungal infections are typically highly virulent and they have the capability of spreading the infection to virtually all bodily organs. Candidiasis, aspergillosis, and cryptococcosis are examples of systemic fungal infections. Cutaneous fungal infections include those that infect the cutaneous tissue including the hair and the nails; athlete's foot, or tinea pedis, is an example of cutaneous fungal infection. Superficial fungal infections affect the host's epidermis; an example of a superficial fungal infection is tinea capitis which is often referred to as a ringworm. Lastly, subcutaneous fungal infections infect all layers of the skin down to the fascia and the muscles such as occur as the result of a deep traumatic puncture wound.
Parasites
Parasites live on or in a host and they get their nutrition from the host. Parasitic infections are most common in tropical third world nations, but they can also occur in some developed countries such as America. Some examples of parasitic infections include pinworms, giardia, tapeworms, lice, maggot infestations, and scabies.
Prions
A prion is not a living organism, instead, it is the abnormal folding of cellular proteins. Prions and prion diseases most often adversely affect the host's brain and neural tissue. Hardy prions, which can only be destroyed with sterilization, are associated with high mortality and high morbidity rates.
Some of the prion diseases include several forms of encephalopathy, including "mad cow" disease, Creutzfeldt-Jacob disease, and other rare diseases such as kuru.
The ability of a pathogenic microorganism to cause infections and diseases and the ability of these microorganisms to cause various degrees of severity depends on a number of factors including a person's physiological condition and susceptibility and the characteristics of the pathogen in terms of its pathogenicity, virulence, and the infective dose.
Pathogenicity is defined as the ability of the pathogenic causative microorganism to actually cause disease. Some pathogens have greater pathogenicity than others. For example, when 1,000 people with the same physiological level of health are exposed to the same pathogen but only 1 develops a disease or infection secondary to this exposure, this pathogen has a lower degree of pathogenicity than when 1,000 people with the same physiological level of health are exposed to the same pathogen and 200 exposed people develop an infectious disease as the result of this exposure.
Virulence is defined and described as how powerful a pathogenic causative microorganism is in terms of its ability to cause disease with a level of severity. Some pathogenic causative microorganisms are more virulent than other pathogenic causative microorganisms.
An infective dose, simply defined, is the amount of the pathogenic causative microorganism that is needed in order to lead to disease and infection. Some pathogenic causative microorganisms need a higher dose than others to cause disease.
In summary, pathogenic causative microorganisms with high levels of virulence, high levels of pathogenicity, and a low infective dose are more threatening than pathogenic causative microorganisms with low levels of virulence, low levels of pathogenicity and a high infective dose.
The Reservoir
The reservoir is the environment within which the pathogen lives, grows, and reproduces. Reservoirs can include humans, animals, water, soil, and insects.
Human Reservoirs
Humans who serve as reservoirs may or may not be adversely affected with infection despite the fact that they serve as the environment within which the pathogenic microorganisms lives, grows, and reproduces as the habitat for the pathogen. For example, asymptomatic carriers like "Typhoid Mary", a cook, was believed to be the first asymptomatic carrier of typhoid, and, as such, it is believed that she infected some 50 plus people. On the other hand, people, including our health care clients, who have active, symptomatic infections, such as influenza, can and do spread and transmit it to others. Additionally, infections can also be spread by an infected person during the incubation period for the specific infection and by convalescent carriers who have recovered from the infection.
Water Reservoirs
Contaminated water is often the reservoir for a number of parasites and other infections like Legionnaires disease, amebiasis, cryptosporidiosis, schistosomiasis, and giardiasis.
Animal Reservoirs
Some animal reservoirs and the infectious disease that they spread include:
- Pigs: Trichinosis
- Cows: Brucellosis
- Rodents: Plague
- Rabbits: Tularemia
- Birds: West Nile encephalitis
- Sheep: Anthrax
- Bats and Dogs: Rabies
Additionally, some diseases such as HIV/AIDS, severe acute respiratory syndrome (SARS), and Ebola have originated in animal reservoirs but now harbor in human reservoirs.
Soil Reservoirs
Many fungal agents, such as those that cause histoplasmosis, live, and multiply in contaminated soil.
Modes of Transmission
Modes of transmission, or transportation, are the part of the cycle of infection that moves a pathogen from its reservoir to its susceptible host. There are several modes of transmission including direct, indirect, airborne, vehicle, and vector modes of transmission.
Direct transmission occurs when a pathogen comes in direct contact with the susceptible host's skin or mucous membrane. Indirect transmission is the movement of an infectious agent from the reservoir to an object which is then passed to the susceptible host when the host touches the object.
Droplet transmission occurs when a pathogen is spread with a spray or splash of infectious microorganisms which can occur with coughing and sneezing for example.
Airborne transmission occurs when the pathogen is carried in dust or droplets in the air. Measles is an example of a virus that is transmitted with the airborne mode of transmission.
Vehicle transmission is defined as contact with an infection in things like contaminated soil and water. Vector transmission is the movement of the pathogen with live things like insects that infect humans with their sting or bite.
The Portal of Exit
The portal of exit is how the pathogenic microorganism leaves the reservoir. For example, influenza leaves the human reservoir with a cough or a sneeze, and Lyme's disease leaves the tick with its infectious bite.
The Susceptible Host
Some patients are more susceptible to and at higher risk of infection than others. Some of the things that increase the patient's or host's susceptibility to infection are high levels of stress, high cortisol levels, old age, infancy, genetics, poor nutrition particularly when the patient is affected with a protein deficit, the presence of physical disorders and diseases, immunosuppression, some medications such as and steroids, and some treatments like radiation therapy and chemotherapy for cancer.
Briefly stated, people get infections when their natural bodily defenses against infection fail. The human body's first line of defense against infection is intact skin. Other bodily defenses include the inflammation process and antibody-mediated defenses including active and passive immunity.
Active immunity is present as a response to an antigen, and passive immunity is present when antibodies to an antigen are present. Both active and passive immunity can be either natural or artificial.
Artificial active and passive immunity is given with an injection of an antibody-like immune globulin which produces artificial passive immunity and the injection of an antigen which reacts with the formation of antibodies against the infection. This is artificial active immunity.
Natural active and passive immunity occurs when the person gets the infection and later produces antibodies against it which prevents future occurrences of this specific infection and when the neonate naturally gets antibodies in utero during pregnancy. These immunities are naturally active and natural passive immunity, respectively.
Periods of Communicability
The period of communicability is defined as the duration of time that a pathogen can indirectly or directly transmit the infection to another. This period of time varies according to the microorganism. Some pathogens are associated with brief periods of communicability and others are characterized with longer periods of communicability.
The Pathogen's Incubation and Latent Periods
The incubation period is the duration of time between the entry of the pathogenic organism into the body upon initial exposure until the signs and symptoms of the infection begin. Pathogens establish themselves in their new environment, they grow, they proliferate and go to their target area during the incubation period of time. All pathogenic microorganisms have incubation periods. Some incubation period is quite long and extended, as is the case with HIV, and others, such as influenza, have a brief incubation period.
Incubation periods vary among pathogenic microorganisms and also among clients. For example, some of the factors that can impact on the duration of the incubation period include the client's physiological state and their level of susceptibility, the microorganism's portal of entry, the dose of the infectious agent, and the speed at which the microorganism replicates. Incubation periods are typically shorter among infants and children and longer among the members of the adult population.
In contrast to incubation periods, which mark the time from initial exposure to signs and symptoms, the latent period of time for pathogenic microorganisms is the period of time between infection and infectiousness, which is the time at which transmission to others is possible.
When the body's defenses against infection are not sufficient to combat it, infections occur. The signs and symptoms of infection, generally speaking, are local and also systemic.
The local signs of infection, like the signs and symptoms of the protective inflammatory process, are site pain, redness, heat, swelling, and some bodily part dysfunction.
The inflammatory process is a protective response that protects and defends us against tissue damage and harm; the inflammatory process and its mechanisms eliminate damaged tissue and promote the restoration of normal bodily tissue.
In the correct sequential order, the phases or stages of this process are:
- The initial tissue injury which can result from an infection or a traumatic cause
- The vascular response. The release of histamine, prostaglandins, and kinins. These substances lead to vasodilation which increases the necessary blood supply to the injured tissue and the area surrounding it.
- The exudate response. The release of leukocytes, including macrophages and neutrophils, to the injured area to combat the infection.
The systemic signs and symptoms of infection include fatigue, chills, hyperthermia, prodromal malaise, tachypnea, tachycardia, nausea, vomiting, anorexia, confusion, incontinence, abdominal cramping, and diarrhea, among other signs and symptoms as based on the infection. For example, urinary infection signs and symptoms can include urgency, dysuria, urinary frequency, and hematuria; and respiratory infections lead to coughing, dyspnea, and adventitious breath sounds.
The Portal of Entry
The portal of entry is the internal or exterior part of the human body that permits the infectious microorganism to enter the human body. For example, many E. coli infections occur when this pathogen enters the susceptible host's mouth. This is called fecal-oral transmission because the pathogen exits via the feces and it enters into the mouth of the susceptible host.
In summary, the chain of infection includes:
- The pathogenic microorganism
- The mode of transmission
- The reservoir
- The portal of exit
- The susceptible host
- The portal of entry
And, the stages of infection are, in correct sequential order:
- The incubation period as discussed above
- The prodromal phase is characterized by fatigue and generalized feelings of malaise and the period of time during which the pathogenic microorganism reproduces.
- The illness stage during which time the client has the symptoms and signs specific to the particular infection
- The convalescence stage which is characterized by the client's recovery from the infection and the cessation of its signs and symptoms
Applying the Principles of Infection Control
The principles of infection control that will be discussed in this section include:
- Asepsis
- Medical asepsis
- Surgical asepsis
- Hand hygiene
- Universal / Standard precautions
- Special transmission precautions and isolation
- The use of personal protective equipment
Asepsis
Asepsis prevents the spread of infection. The two types of asepsis are medical asepsis, or clean procedure, and surgical, or sterile, asepsis.
Some of the basic principles relating to asepsis are:
- Some treatments and procedures require surgical asepsis and others only require medical asepsis.
- Skin, including that on the hands, cannot be sterilized; they can only be sanitized.
- Nurses and other health care providers must stop all procedures and treatments and then begin all over again whenever a break in surgical asepsis or medical asepsis occurs.
- Nurses, including licensed practical and registered nurses, can perform treatments and procedures that require surgical and/or medical asepsis. Nursing assistants and other unlicensed assistive staff cannot perform treatments or procedures that require surgical asepsis; these unlicensed staff can only perform treatments or procedures that require medical asepsis.
Medical Asepsis
Medical asepsis also referred to as a clean technique, is the infection control principle and practice that decreases the spread of infection. Medical asepsis reduces the number of pathogenic microorganisms and it also impairs the proliferation and growth of microorganisms.
Hand hygiene, skin preparation prior to the injection of a subcutaneous medication, and the administration of all medications except those given intravenously are examples of the application of medical asepsis principles into nursing care practices.
Surgical Asepsis
Unlike medical asepsis, surgical asepsis, also referred to as surgical technique, eliminates all microorganisms.
The principles and techniques of surgical asepsis are applied when the skin is not intact and also when internal areas of the body are being entered, cared for, or treated. Surgical asepsis is used for wound care, during all invasive procedures including surgical procedures and other invasive procedures such as endoscopy, for the administration of intravenous medications, for wound care, and for the insertion of an indwelling urinary catheter as well as other internally placed tubes like central lines and peripheral intravenous lines.
Hand Hygiene
Handwashing is the best and most effective way to prevent the spread of infection when it is done correctly and properly. Proper handwashing can be done with friction and regular soap and water or special alcohol-based hand sanitizing antimicrobial solution, for at least 20 seconds.
Handwashing is particularly important in the health care environment for many reasons including the fact that health care facilities are highly prone and susceptible to many healthcare-acquired infections, including those such as like methicillin-resistant staphylococcus aureas (MRSA), vancomycin-resistant enterococcus (VRE), and penicillin-resistant Streptococcus pneumoniae, which are highly resistant to antimicrobial treatment. Please note, although special alcohol-based hand sanitizing antimicrobial solutions are effective against most pathogenic microorganisms, they are not effective against Clostridium difficile (C. diff).
Handwashing is done using friction for a minimum of twenty seconds before and after each client contact, in addition to other times such as before and after donning and removing gloves.
Alcohol-based hand cleansers are not a substitute for good handwashing, however, they can be used when running water and soap are not accessible. Alcohol-based handwashing products are liberally applied to the entire hand after which the hands are rubbed until the entire hand is dried completely.
Universal / Standard Precautions
Universal and standard precautions are infection control measures that are used to prevent the spread of infection among ALL patients whether or not they have a known infection. Standard precautions protect health care workers and patients from the spread of infection secondary to contaminated blood and other bodily fluids.
Special Transmission Precautions and Isolation
Contact precautions prevent direct and indirect contact transmissions of infectious pathogens like those found in infected wounds, infectious diarrhea, and infections such as herpes simplex; droplet precautions are used to prevent the transmission of pathogens that are transmitted with a cough or sneeze, therefore, face masks are indicated for these precautions; and airborne precautions are used for airborne transmission microbes like tuberculosis which requires a negative pressure private room and a HEPA mask.
Personal Protective Equipment
The use of personal protective equipment protects the health care staff, clients, and visitors against infections. Personal protective equipment (PPE) is specialized equipment and attire that is used by employees in health care to protect against infections. Examples of personal protective equipment include gowns, gloves, masks, goggles, and respirators.
Some basic principles for donning and removing personal protective equipment include donning sterile gowns and gloves using the surgical technique by touching only the sterile surfaces of these items with sterile hands. For example, the first sterile glove is applied by touching the inside of the glove with the bare hand after which the second sterile glove is donned by holding the glove with the sterile gloved hand without touching any skin surfaces.
Another basic principle includes removing used personal protective equipment by folding the item inside out and disposing of it in the proper receptacle.
Using Appropriate Technique to Set up a Sterile Field and Maintaining Asepsis
These basic sterile asepsis procedures are followed for setting up and maintaining a sterile field.
- Sterile items ONLY are placed on the sterile field.
- The nurse must NEVER turn their back to a sterile field.
- The nurse must NEVER lean over a sterile field.
- The nurse must NEVER have the sterile field below the waist level.
- Coughing or sneezing over the sterile field contaminates the sterile field.
- The nurse must maintain a one-inch border around the sterile field that is not sterile.
- All sterile items and supplies are put inside of this one-inch border.
- The sterile field must remain dry; any wetness or moisture contaminates the sterile field.
- Sterile liquids must be poured carefully into sterile containers on the sterile field without the solution running over and obliterating the label on the bottle.
- Sterile gowns and gloves are used by staff that is working with and/or setting up a sterile field.
- Sterile masks are also indicated, particularly when there is a possibility that a person will be working with or near the sterile field.
Whenever these things are NOT done and maintained continuously throughout the treatment or procedure, the entire sterile field and its contents are promptly discarded because the sterile field is no longer sterile. The entire set up must be redone from the very beginning.
Following the Correct Policy and Procedures When Reporting a Client With a Communicable Disease
All states have laws and regulations that mandate the reporting of communicable diseases, most of which must also be reported to the Centers of Disease and Prevention. The purpose of this reporting is to facilitate the tracking and trending of communicable diseases and epidemics in order to reverse the threat and to prevent future outbreaks. It is the responsibility of health care to report communicable diseases and not the responsibility of the client or the family member.
Some of this mandatory reporting can be done with a telephone call and other communicable disease occurrences must be reported with a written report.
Some of the communicable diseases that must be reported include anthrax, salmonella, gonorrhea, pertussis, and rubella.
Educating the Client and Staff Regarding Infection and Infection Control Measures
As with other education, registered nurses assess the educational needs of both staff and clients, they plan educational activities to meet these assessed needs, they provide the education and they also evaluate the outcomes of these educational activities in terms of their effectiveness.
The assessment of these needs can be direct or indirect. For example, a registered nurse may directly observe improper handwashing being done by another staff member and they can indirectly assess educational needs when they collect, aggregate, and analyze data relating to the frequency of infections.
Some of these educational needs are within the cognitive domain of learning and others are within the psychomotor domain of learning. For example, a client may indicate that they have a cognitive learning need when they ask why they are isolated into a private room; and a visitor may indicate that they have a psychomotor learning need when you observe the discarding of their gown and mask outside of the client room.
Once educational needs are assessed, educational activities are planned and implemented in order to meet these needs.
Some of the content that is typically presented to clients and staff members and according to their level of understanding can include:
- The chain of infection
- Ways to prevent infection by breaking the chain of infection
- Surgical and medical asepsis
- The use of personal protective equipment (PPE)
- Handwashing
- Standard/Universal precautions
- Special transmission-based precautions and practices
- The handling and disposal of biohazardous waste
- Immunity and immunization schedules
Utilizing Appropriate Precautions for Immunocompromised Clients
The client's immune system protects it from infection. Immunocompromise, in addition to the other intrinsic risk factors, such as a very young age and advancing years, some medications, some disorders such as HIV/AIDS, poor nutritional status, and therapeutic interventions such as radiation therapy and chemotherapy, place clients in varying degrees of risk in terms of contracting an infection.
Protective precautions, in addition to standard/universal precautions, may be necessary when a client is significantly and adversely affected with immunocompromised and/or a circumstance such as being an organ transplantation recipient. Protective precautions reduce the risk of infection by separating the immunocompromised client from microorganisms including those that do not normally affect a person without immunocompromise. For example, clients with HIV/AIDS are protected from microorganisms that do not normally affect a person without immunocompromised. Protective isolation prevents these opportunistic infections among clients affected by HIV/AIDS.
Evaluating Infection Control Precautions That Are Implemented by Staff Members
Nurses, directly and indirectly, evaluate staff competency in terms of their utilization of infection control measures and precautions, such as those within the cognitive domain of learning and the psychomotor domain of learning as listed above under the topic "Educating the Client and Staff Regarding Infection and Infection Control Measures".
Evaluating Whether Aseptic Technique is Performed Correctly
Again, nurses, directly and indirectly, evaluate staff competency in terms of their utilization of infection control measures and precautions including their correct performance of the aseptic technique.
RELATED CONTENT:
- Accident/Error and Incident Prevention
- Emergency Response Plans
- Ergonomic Principles
- Handling Hazardous and Infectious Materials
- Home Safety
- Reporting Incident/Event/ Irregular Occurrence/Variances
- Safe Use of Equipment
- Security Plans
- Standard Precautions/Transmission Based Precautions/Surgical Asepsis (Currently here)
- Use of Restraints/Safety Devices
SEE – Safety & Infection Control Practice Test Questions
