What you’ll learn in this article…
- Epic holds over half of all U.S. staffed hospital beds in 2026.
- Nurses typically need three to six months for true EHR proficiency.
- AI ambient documentation is moving from pilot programs into mainstream use.
Nurses spend between 25 and 40 percent of each shift documenting patient care, a reality that makes the charting system one of the most influential tools in clinical practice. The platform a hospital selects determines how quickly you can find a patient's medication history, whether flowsheets auto-populate or require manual entry, and how much cognitive load remains after a 12-hour shift.
Charting technology has consolidated rapidly. Epic Systems now holds more than half of all staffed hospital beds in the United States, yet MEDITECH, Oracle Health, and dozens of specialty platforms still serve distinct facility types and unit needs. Understanding where the market stands, how costs actually break down, and what emerging AI features mean for bedside documentation gives nurses leverage in conversations about workflow, training, and resource allocation.
What Are Nursing Charting Systems? EMR Vs. EHR Explained
Electronic medical records confined to a single practice versus electronic health records designed to travel across an entire care network: the distinction sounds like IT jargon, but it has real consequences for every nurse who documents at the bedside.
EMR vs. EHR: What the Terms Actually Mean
An EMR (electronic medical record) is the digital version of the paper chart that used to live in a clipboard at the foot of a patient's bed. It stores clinical data, such as vitals, progress notes, and lab results, within one practice or facility. If a patient transfers to another hospital system, the EMR typically does not follow.
An EHR (electronic health record) is broader in scope. It is built for interoperability, meaning it can share patient information across hospitals, specialists, pharmacies, and labs. Most large health systems now operate on EHR platforms, and the terms EMR and EHR are often used interchangeably in everyday conversation, even though their technical capabilities differ.
For bedside nurses, the practical takeaway is this: an EHR makes it easier to view a patient's full history, including outside records, medication reconciliation data, and discharge summaries from prior admissions. An EMR may limit that visibility to only the encounters documented in your own facility.
Why Charting Systems Are a Nursing Concern
Nurses are the heaviest users of any charting platform. The components that matter most to direct-care nurses live deep inside these systems:
- Flowsheets: Where you document vitals, intake and output, neuro checks, and other time-stamped assessments throughout a shift.
- Medication Administration Records (MARs): The interface for scanning barcodes, verifying doses, and documenting administration times.
- Care Plans: Templates that map nursing diagnoses to interventions and expected outcomes.
- Nursing Assessments: Head-to-toe documentation modules that vary significantly from one vendor to the next.
Because nurses interact with these tools for a large portion of every shift, the design, speed, and logic of a charting system directly affect workflow, patient safety, and even job satisfaction. Nurses interested in shaping how these systems are built and implemented may find that nursing informatics degree programs provide a focused pathway into that work.
From Paper to Digital: A Brief Timeline
The shift from paper charting to digital documentation accelerated after the HITECH Act of 2009, which incentivized hospitals to adopt certified EHR technology. By the mid-2010s, the vast majority of U.S. hospitals had transitioned to electronic systems. However, the nursing experience with those systems varies enormously depending on the vendor, the facility's customization choices, and how much input nurses had during implementation. Some units run on streamlined, intuitive builds; others work with cluttered templates that require dozens of clicks for a single assessment.
What Charting Formats Do Most Hospitals Use?
Regardless of the software vendor, nursing documentation generally follows one of several established formats:
- SOAP notes: Subjective, Objective, Assessment, Plan. Common in outpatient and primary care settings.
- Narrative charting: Free-text entries that describe events in chronological order, still used in some emergency and psychiatric settings.
- Flowsheet-based charting: The dominant method in acute care, where nurses document data points at timed intervals using structured fields.
- Charting by exception: Nurses document only findings that deviate from an established baseline, reducing redundant entries.
Most hospital-based nurses will encounter flowsheet-driven documentation as their primary format, supplemented by narrative notes for events that fall outside structured fields. Later sections of this guide compare these formats in greater detail and outline how different EHR vendors handle each one.
Top EMR and EHR Systems Used by Nurses: Market Share and Adoption
Epic Systems commands the acute care hospital charting landscape, capturing more than half of all staffed hospital beds in the United States and securing roughly seven out of every ten new hospital EHR contracts.1 Market share shifts dramatically by facility size and care setting, however, meaning the system a nurse encounters at a 600-bed academic medical center will differ from the charting tool in a 25-bed rural hospital, an independent surgical center, or a home health agency.
Market Share Snapshot: Who Dominates Hospital Charting
Epic holds 42.3 percent of acute care hospitals and 54.9 percent of acute care beds, a lead driven by its adoption among large health systems and academic medical centers.1 Oracle Health, the second-largest vendor after acquiring Cerner, accounts for 22.9 percent of hospitals and 22.1 percent of beds, with installations concentrated in medium-to-large acute facilities.1 MEDITECH captures 14.8 percent of hospitals but only 12.7 percent of beds, reflecting its strength in small and community hospitals, particularly in rural markets where lower licensing costs and simpler implementation timelines align with smaller IT budgets.1
In ambulatory settings, the picture changes: eClinicalWorks leads with 11.9 percent of the outpatient market, followed by Epic at 19.5 percent (buoyed by health systems extending their inpatient platform into outpatient clinics), athenahealth at 6.9 percent, and Allscripts at 3.1 percent.2 Oracle Health trails at 5.4 percent in ambulatory, a reflection of Cerner's historically acute care focus.2
Charting Systems by Care Environment
Nurses moving between specialties will encounter different platforms. Epic dominates intensive care and operating room charting in large hospitals, where its tightly integrated clinical decision support and real-time documentation align with fast-paced, high-acuity workflows. MEDITECH appears more often in community hospital medical-surgical units and emergency departments. Nurses working in rural nursing settings should be aware that home health and long-term care markets remain fragmented across dozens of specialty vendors, many of which nurses will not recognize from their hospital training.3
Athenahealth and eClinicalWorks serve primarily independent physician practices and small ambulatory clinics, meaning nurses in outpatient infusion centers, family practice offices, or urgent care often work with these lighter-weight systems rather than the Epic or Oracle platforms they used in acute care.
Nurse-Focused Feature Highlights by Vendor
- Epic: Real-time interoperability across departments, comprehensive medication reconciliation, and robust mobile charting through Haiku and Rover apps.
- Oracle Health (Cerner): Customizable flowsheet templates, strong ambulatory integration post-acquisition, and wide third-party device connectivity.
- MEDITECH: Intuitive web-based interface (Expanse platform), lower cost of ownership for smaller facilities, and straightforward regulatory reporting.
- athenahealth: Cloud-native design with automatic updates, embedded patient engagement tools, and streamlined billing workflows for outpatient nurses.
- eClinicalWorks: Fast charting shortcuts for high-volume primary care, telehealth integration, and population health dashboards.
Market Share Does Not Equal Best Fit
A vendor's bed share tells you which system you are statistically most likely to encounter during your career, not which one will make your shift easier. Usability at the bedside, alignment with your specialty's charting patterns, and the quality of your facility's implementation and training matter more than national rankings. A well-configured MEDITECH installation in a community hospital can outperform a poorly customized Epic rollout in a tertiary center if the workflows match how nurses actually document.
Questions to Ask Yourself
How to Compare Charting Systems: Key Features Nurses Should Prioritize
Epic Systems holds a 2026 overall performance score of 8.5 out of 10 from KLAS Research, placing it ahead of MEDITECH Expanse at 7.8 and Oracle Health at 6.8.1 Those numbers give you a starting benchmark, but they reflect aggregated responses across roles and settings. The features that matter most to a floor nurse differ substantially from what a nurse manager or an informatics specialist needs, so any useful comparison has to get more specific.
A Decision Checklist by Role
Floor nurses live in the documentation moment: they need low click counts to complete routine tasks, fast flowsheet entry, and a medication administration record that integrates cleanly so they are not toggling between screens mid-workflow. Bedside device support, including wall-mounted workstations, workstations on wheels, and tablet access, directly affects how much time nurses spend walking away from patients to chart.
Nurse managers care about a different layer. Customizable care plan templates, staffing dashboards, and the ability to pull audit trails quickly matter more than raw charting speed. Interoperability with other hospital systems, including lab, pharmacy, and scheduling, affects how much manual reconciliation their teams carry.
Informatics nurses need the deepest flexibility: support for standardized nursing language such as NANDA diagnoses, NIC interventions, and NOC outcomes, plus reporting tools that can surface documentation quality metrics and identify workflow bottlenecks. Advanced practice APRN careers in nursing often intersect with informatics responsibilities, particularly as clinical documentation roles expand.
Specialty-Specific Workflows
Not every unit charts the same way, and a system that works for a medical-surgical floor may fall short in a specialty context.
- ICU: Real-time drip calculations and continuous monitoring integration are non-negotiable. Charting delays in a critical care environment carry direct patient safety implications.
- Operating room: Count sheets, implant logs, and surgical safety checklists require structured templates that general flowsheets do not always accommodate.
- Home health: Offline capability is essential because nurses frequently work in areas with unreliable connectivity. Data must sync accurately when a connection is restored.
- Long-term care: Integration with the Minimum Data Set process is a practical requirement, not a nice-to-have. Systems that handle MDS workflows internally reduce duplicate data entry.
How the Major Vendors Compare
Based on available 2026 performance data and general clinical informatics knowledge, here is a high-level comparison across six feature dimensions.1
- Usability scores: Epic's estimated usability score ranges from 55 to 65, MEDITECH Expanse from 48 to 58, and Oracle Health from 40 to 50. No vendor in this group clears a score that usability researchers would consider high, which reflects a persistent industry-wide documentation burden problem.
- Nurse satisfaction: Epic is rated above average, MEDITECH moderate, and Oracle Health below average in 2026 assessments. Nurse satisfaction tends to track closely with click efficiency and flowsheet design.
- Flowsheet customization: Epic offers extensive template customization, which is one reason larger health systems favor it despite higher implementation costs. MEDITECH Expanse has improved its configuration options in recent versions. Oracle Health's customization layer has drawn more criticism for requiring significant IT involvement to adjust.
- MAR integration: All three platforms include medication administration record functionality, but tightness of integration with pharmacy and barcode scanning varies by implementation and facility configuration.
- Standardized nursing language: Support for NANDA, NIC, and NOC terminology exists across platforms but is often an add-on or requires deliberate configuration. It is worth asking vendors for a specific demonstration during evaluation.
- Interoperability: Epic's network has the broadest reach for external record sharing. Oracle Health has a large installed base in government and VA settings. MEDITECH Expanse has invested in FHIR-based interoperability but tends to have a stronger footprint in community and critical access hospitals.
When evaluating any system, request a live workflow demonstration using the specific unit type your nurses work in, not a generic demo environment. The gap between a polished sales demo and daily clinical use is where most dissatisfaction originates.
Related Articles
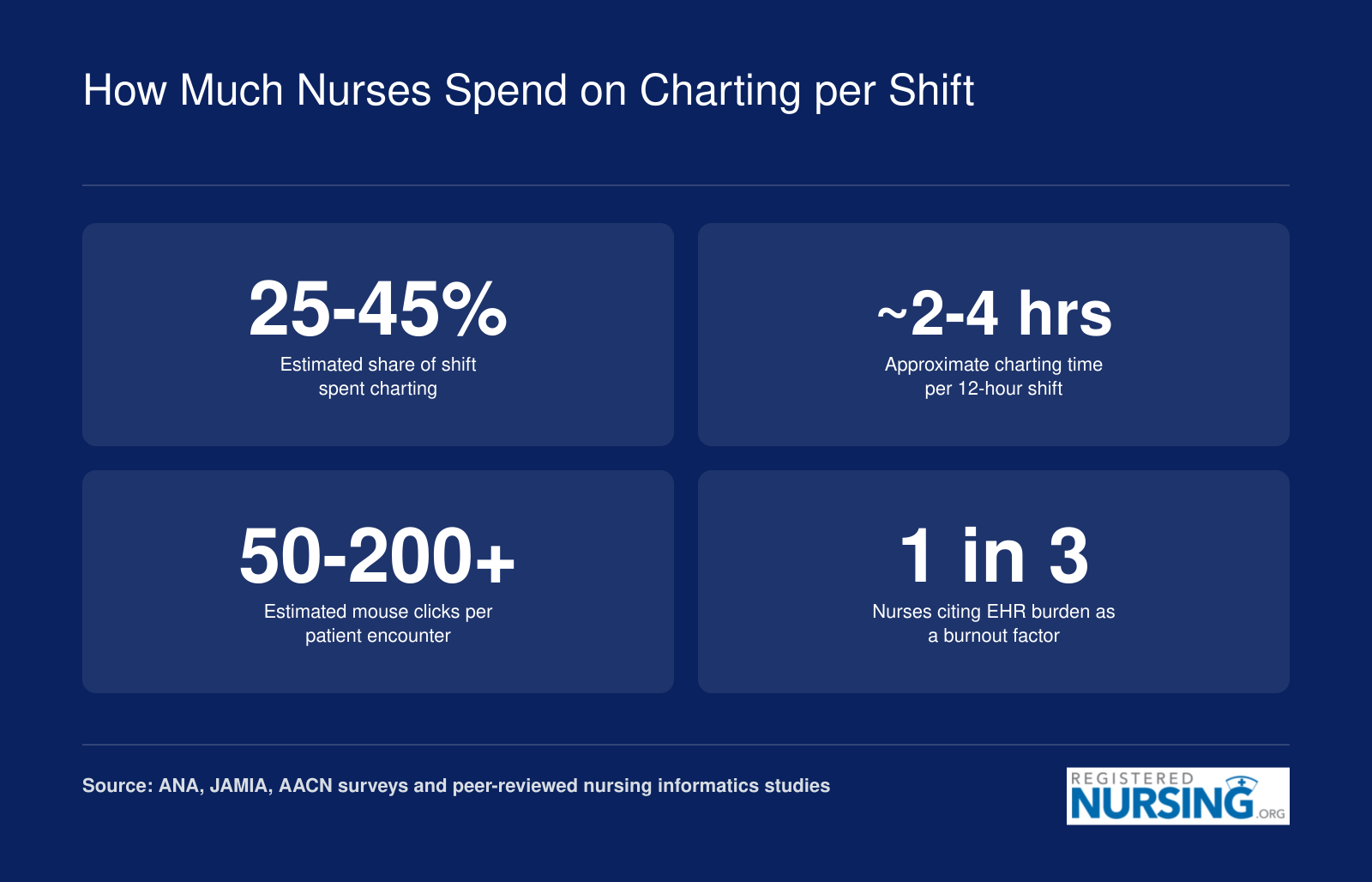
How Much Nurses Spend on Charting per Shift
Documentation is one of the most time-intensive parts of a nursing shift. While exact figures vary by specialty, facility type, and charting system, research from nursing organizations and informatics journals consistently highlights how much of a nurse's workday goes to the screen rather than the bedside. Below are commonly cited estimates drawn from professional surveys and peer-reviewed studies.
AI and Emerging Technology in Nursing Documentation
Artificial intelligence is reshaping how nurses chart, and the pace of change between 2025 and 2026 has been faster than many clinicians expected. Ambient listening, natural language processing, and generative AI are all moving from pilot programs into mainstream EHR platforms, with direct implications for how much time nurses spend documenting care.
How Ambient AI Documentation Works at the Bedside
Ambient AI tools use microphones and natural language processing to "listen" during patient encounters, then draft clinical notes automatically. Products like Nuance DAX Copilot and Dragon Medical One have offered this capability for physicians for several years, and Nuance DAX Copilot now integrates natively with Epic for enterprise-scale deployment.1 In February 2026, Epic launched its own native ambient AI scribe embedded directly within the EHR, eliminating the need for third-party add-ons in many workflows.2
For nurses specifically, Epic has rolled out AI-powered features targeting end-of-shift documentation, an area that historically consumes significant unpaid time.3 Early data from Epic customers suggests that ambient AI documentation can reduce charting time by roughly 50 percent, with some clinicians reporting savings of one to four hours per day.4 Epic's own reporting indicates documentation time reductions of up to 85 percent for nursing-specific use cases, though these figures come from early adopter sites and may not reflect every clinical setting.3 As of mid-2025, over 62 percent of Epic customers had adopted ambient AI features,4 and approximately 85 percent had adopted some form of Epic's AI Copilot tools.5
NLP-Driven Auto-Suggestions for Nursing Assessments
Beyond ambient listening, generative AI is being woven into assessment and care plan workflows. Oracle Health has deployed clinical AI agents across roughly 30 specialties, with tools that suggest nursing assessments, flag inconsistencies, and pre-populate care plan elements based on patient data.4 Epic's generative AI features similarly offer auto-suggestions that nurses can accept, modify, or reject during charting. Early accuracy benchmarks for ambient AI-generated notes hover around 98 percent, though accuracy varies by clinical context and documentation type.1
Privacy, Accuracy, and the Nurse's Review Role
AI-generated documentation must comply with HIPAA, and the major platforms process data within encrypted, access-controlled environments. However, clinical validation of AI-drafted notes remains the nurse's responsibility. No regulatory body currently certifies AI-generated nursing documentation as a standalone legal record. Every note produced by ambient AI or generative suggestions requires a human review step before it becomes part of the patient chart. Nurses should treat AI output as a draft, not a finished product, verifying clinical details against their own observations and the patient's record.
Key concerns to keep in mind:
- Accuracy verification: AI may misinterpret clinical terminology, ambient noise, or context-specific language, especially in high-acuity or fast-paced settings.
- HIPAA compliance: Confirm that your organization's AI tools process and store data in environments that meet federal privacy requirements.
- Scope of validation: No current AI charting tool has received FDA clearance or equivalent regulatory validation for autonomous clinical documentation.
The Gap: Nurse-Specific AI Is Still Catching Up
Most ambient AI and generative documentation tools were designed with physician workflows in mind. Physician notes tend to follow more predictable structures, making them easier targets for natural language processing. Nursing documentation, which spans flowsheets, assessments, interventions, and narrative notes across entire shifts, presents a more complex challenge for AI models.
That gap is closing. Epic's 2026 releases specifically target nursing workflows, including end-of-shift summaries and assessment documentation.3 Oracle Health and third-party developers are also expanding their tools to address nursing-specific charting patterns. Still, nurses evaluating AI features today should ask whether a given tool was trained on nursing documentation or primarily on physician encounter notes, because the distinction matters for accuracy and usability.
The trajectory is clear: AI will handle an increasing share of documentation labor. Nurses who want broader context on how these tools fit into the profession can explore AI in nursing for a wider look at what these changes mean for future practice. In 2026, the technology works best as a time-saving assistant rather than a replacement for clinical judgment. Nurses who learn to review and refine AI-generated notes efficiently will be well positioned as these tools mature.
Charting System Costs: What Healthcare Organizations Actually Pay
The tension between budget constraints and clinical functionality defines every EHR purchasing decision, forcing organizations to weigh upfront savings against long-term usability and total cost of ownership. Understanding how pricing actually works helps nurses advocate for the resources their units need rather than accepting inadequate technology as a fixed limitation.
Pricing Models: How Vendors Structure Their Fees
Healthcare organizations encounter several distinct pricing structures when evaluating charting systems.4 Per-provider or per-seat licensing charges a monthly or annual fee for each clinician with system access, common among ambulatory-focused vendors. Enterprise site licenses cover an entire organization for a negotiated flat fee, typical of large inpatient deployments. Cloud-based subscription models (SaaS) bundle hosting, maintenance, and updates into recurring payments, reducing upfront capital requirements. Many organizations end up with hybrid arrangements combining elements of each approach.
Ambulatory practices see monthly per-provider costs ranging from $99 to $199 for basic systems up to $349 to $449 for premium platforms.3 A mid-range example: athenahealth athenaOne starts around $140 per provider monthly at minimum, though a 20-provider group might pay closer to $1,350 per provider monthly depending on services included.2 eClinicalWorks prices its EHR-only package at $449 per provider monthly, rising to $599 with practice management features.1 Some vendors charge percentage-based fees on collections instead, with athenahealth taking 4 to 7 percent and eClinicalWorks charging 2.9 percent for revenue cycle management services.1
Implementation Costs by Organization Size
The gap between a small clinic and a large health system is staggering. Small practices typically spend $5,000 to $15,000 annually per provider on their EHR, including implementation and ongoing costs. Data migration alone runs $1,000 to $3,000 per practice.5
Mid-size regional health systems face total program costs of $50 million to $150 million for enterprise EHR implementations. Large academic medical centers and integrated delivery networks routinely invest $300 million to $500 million for comprehensive deployments.5 At this scale, EHR spending represents 2 to 5 percent of annual operating revenue as an ongoing commitment.
Total Cost of Ownership Beyond the License Fee
The sticker price captures only a fraction of actual expenses. Training represents a substantial investment, both in direct costs and the productivity loss while staff learn new workflows. Hardware requirements add up quickly: bedside devices, workstations on wheels, barcode scanners, and the infrastructure to support them. Ongoing maintenance contracts, mandatory upgrades, interface development for connecting ancillary systems, and customization fees to match clinical workflows all contribute to long-term spending.
athenahealth charges $2,000 to $5,000 per provider just for implementation, separate from monthly subscription costs.2 Enterprise systems require dedicated IT staff, project managers, and often external consultants throughout multi-year rollouts.
Hidden Costs Nurses Should Advocate For
Budget decisions made without frontline input often create problems nurses live with daily. When organizations skimp on device quantity, nurses waste time hunting for available workstations or waiting for colleagues to finish charting. Inadequate superuser training leaves units without go-to experts when problems arise. Insufficient workflow customization forces nurses into time-consuming workarounds that compound across every shift.
Nurse leaders should push for adequate device-to-nurse ratios during purchasing discussions, ongoing training budgets rather than one-time onboarding, and dedicated customization resources to address unit-specific needs. The cheapest implementation often becomes the most expensive when measured in nursing hours lost to inefficient systems.
The sticker price of an EHR often represents less than half the true cost. Training, hardware upgrades, customization, workflow redesign, and productivity loss during go live can double or triple the initial investment. Nurses and nurse leaders evaluating systems should always ask vendors about total cost of ownership across three to five years, not just annual licensing fees.
Training and Onboarding: How Long It Takes Nurses to Learn a New Charting System
Vendor-led classroom training versus daily hands-on practice: most hospital EHR training programs deliver 8 to 20 hours of formal instruction, but nurses consistently report that true proficiency takes three to six months of real-world charting. Epic nursing staff typically complete 6 to 12 hours of initial training,1 while UCHealth onboards new nurses in approximately 2 to 3 hours of focused classroom time.1 Epic physicians receive about 10 hours of classroom instruction plus 4 hours in learning labs.2 The gap between formal training and workflow fluency is where superuser programs, sandbox practice, and specialty-specific modules make or break adoption success.
How Vendor Training Resources Compare
Epic operates a formal credentialing program that trains hospital-based instructors over a six-week period,2 creating an internal cadre of certified trainers who can tailor onboarding to unit needs. Epic also offers Nursing SmartUser Classes, a series of 4 one-hour webinars designed to deepen charting skills beyond the basics,3 and expects nursing staff to complete 3 to 5 hours of ongoing training each year.1 Oracle Health (formerly Cerner) provides a centralized learning portal with on-demand modules, while MEDITECH emphasizes vendor-supported implementation teams that work alongside hospital educators during go-live events.
The superuser or champion model accelerates unit-level adoption by embedding peer mentors who have completed advanced training and can answer questions at the bedside during the first weeks of a new system. These champions bridge the gap between IT support and clinical workflow, offering tips on documentation shortcuts, order-entry sequences, and where to find buried features that classroom trainers may not cover.
Practical Tips for Learning a New Charting System
Volunteer as a superuser if your hospital offers the role: you will receive deeper training, early access to the system, and a voice in customization decisions. Build your own quick-reference sheets with screenshots of frequently used screens, reminder lists for specialty-specific charting (such as hemodynamic parameters in critical care or pain reassessment intervals in oncology), and workarounds for common errors. Spend time in the sandbox or test environment, where you can practice documentation without affecting live patient records. Ask for workflow training tailored to your specialty rather than relying solely on generic nursing modules; medication reconciliation for a pediatric oncology nurse looks different from that of an orthopedic floor nurse.
What New Graduates Should Expect
Nursing schools increasingly incorporate simulated EHR training into clinical courses, with many programs using Epic or Oracle Health practice environments so students can log assessments, orders, and care plans before graduation. Some schools require students to complete 3 to 4 hours of pre-clinical EHR training and achieve a 90 percent passing score on competency tests.4 New graduates who have charted in a school-based simulator still face a learning curve during hospital orientation because live systems include organization-specific customizations, integrated medication dispensing devices, and unit protocols that simulations cannot replicate. Expect your first month on the floor to involve frequent clarifications, duplicate documentation checks, and requests for help navigating unfamiliar screens.
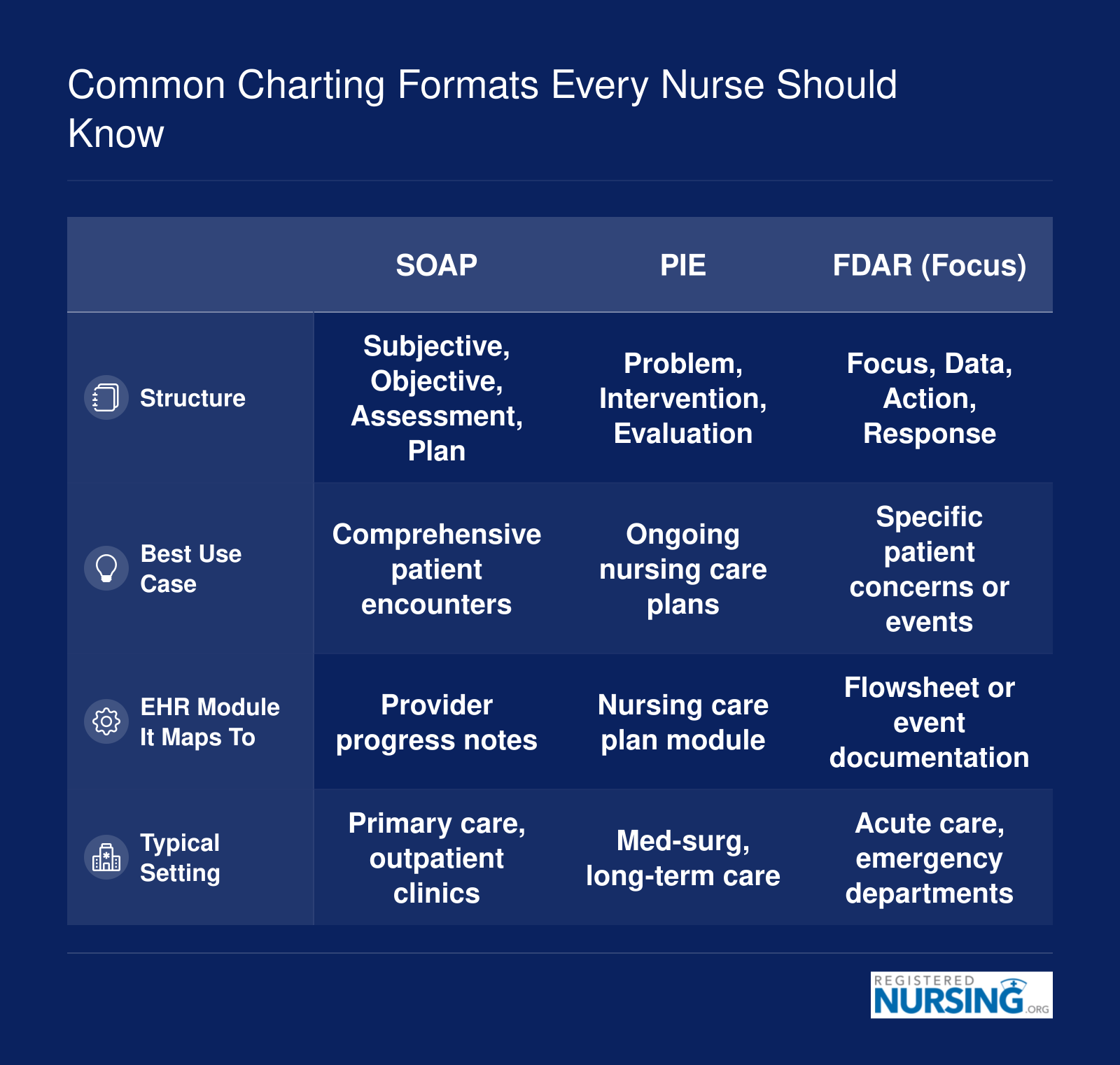
Common Charting Formats Every Nurse Should Know
Nurses encounter several standardized documentation formats depending on their clinical setting and the EHR platform in use. Each format organizes patient information differently, and knowing how they compare helps you chart faster and more accurately. Here is a side-by-side look at the four most widely used charting formats.
Frequently Asked Questions About Nursing Charting Systems
Nurses frequently have questions about charting systems, whether they are evaluating options for a new facility or trying to get the most out of the platform they already use. Below are answers to the most common questions about EMR and EHR solutions in nursing practice.
- What is the best charting system for nurses?
- There is no single best charting system for every nurse. Epic consistently ranks highest in nurse satisfaction surveys due to its intuitive workflow and comprehensive clinical tools. However, the best system depends on facility size, specialty, and budget. Oracle Health (formerly Cerner) and MEDITECH are also widely used and well regarded. The ideal choice balances usability, interoperability, and support for nursing workflows.
- What is the difference between EMR and EHR in nursing?
- An EMR (electronic medical record) is a digital version of a patient's chart within a single practice or facility. An EHR (electronic health record) goes further by allowing information to be shared across multiple healthcare organizations and providers. In nursing, the distinction matters because EHR systems support care coordination, enabling nurses to access a patient's full history regardless of where previous care was delivered.
- How long does it take nurses to learn a new charting system?
- Most nurses need four to eight weeks of combined classroom training and supervised practice to become proficient with a new charting system. Basic navigation can be learned in a few days, but building the muscle memory for efficient documentation during a busy shift takes longer. Facilities that offer ongoing support, super users, and tip sheets tend to see faster adoption and fewer errors.
- How does AI improve nursing documentation?
- AI improves nursing documentation by automating repetitive tasks such as populating flowsheets, suggesting clinical phrases, and transcribing verbal notes through ambient listening technology. Some systems use natural language processing to convert narrative notes into structured data. This reduces the time nurses spend charting, lowers the risk of documentation fatigue, and helps ensure more accurate, complete records.
- What charting format do most hospitals use?
- Most hospitals use a combination of structured templates and narrative documentation within their EHR. Common formats include SOAPIE (Subjective, Objective, Assessment, Plan, Intervention, Evaluation), DAR (Data, Action, Response), and focus charting. Many facilities also rely on exception-based charting, where nurses document only deviations from established norms, which saves time while still capturing clinically relevant information.
- Can nurses customize their EHR flowsheets?
- In most modern EHR systems, nurses can personalize certain elements of their flowsheets, such as reordering columns, creating favorites, or building quick-text shortcuts. However, the degree of customization depends on the platform and facility policies. System administrators typically control the overall structure, while individual nurses can adjust views and templates within those parameters to match their workflow preferences.
- Is Epic harder to learn than Cerner?
- Neither system is inherently harder to learn, but nurses often report that Epic feels more intuitive out of the box due to its consistent interface design. Oracle Health (Cerner) offers extensive customization, which can feel overwhelming at first but becomes powerful once mastered. Learning difficulty depends more on the quality of your facility's training program and the complexity of your unit's specific build than on the software itself.
- What is the most affordable EHR for small practices?
- For small nursing practices and clinics, cloud-based EHR platforms such as athenahealth, eClinicalWorks, and DrChrono tend to be the most affordable options. Many offer subscription pricing that starts at a few hundred dollars per provider per month, with lower upfront costs compared to enterprise systems like Epic or Oracle Health. Some also include revenue cycle management tools, which can offset the subscription expense.