What you’ll learn in this article…
- Paper medication records are linked to error rates of 2.8 to 16 percent.
- HIPAA compliance rules apply equally to paper and electronic health records.
- Hybrid transition strategies reduce risk when moving from paper to EMR.
Despite widespread EMR adoption, a 2025 survey by the American Medical Association found that nearly one in five primary care practices still uses some form of paper documentation, a share that climbs higher in rural clinics, small long-term care facilities, and specialty practices with fewer than five providers. For nurses and administrators in those settings, the question is not whether paper records are outdated in theory but whether they remain practical given real-world constraints like upfront cost, IT support availability, and workflow stability.
Paper charting persists because it requires no software licensing, no server infrastructure, and no training budget. At the same time, it carries measurable disadvantages in error rates, retrieval speed, and HIPAA compliance guidance for physical records. The tension between upfront affordability and long-term liability shapes how small practices and rural facilities approach documentation today.
What Are Paper Medical Records?
What exactly counts as a "paper medical record," and where do nurses still encounter them in 2026?
A paper medical record is any patient health document created, stored, and retrieved in physical form rather than through a digital system. That umbrella covers handwritten progress notes, printed lab results, physician orders, nursing assessments, medication administration logs, consent forms, and discharge summaries, all filed in a paper chart or folder. The record lives in a physical space, whether a manila folder at a rural clinic or a locked filing cabinet in a correctional facility.
A Brief History of the Paper Chart
For most of modern medicine, paper was the only option. Nurses learned to chart on paper, and hospitals built entire medical records departments around it. That began to shift after the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 offered financial incentives to healthcare organizations that adopted certified electronic health record systems. Adoption accelerated quickly among hospitals and large group practices. Even so, a meaningful share of small and solo practices, along with certain specialty settings, continued using paper or hybrid systems well into the 2020s, a pattern that has not fully disappeared.
Where Nurses Still Encounter Paper Charting
Paper records are not a relic. Nurses working in the following settings are particularly likely to encounter them, or at least some version of a hybrid workflow:
- Rural and federally qualified health clinics: Limited IT infrastructure and budget constraints slow full EMR adoption. Nurses who pursue rural nursing careers should expect to navigate paper-based workflows more often than their hospital counterparts.
- Behavioral health and psychiatric facilities: Some states permit or require specific paper-based consent and treatment documentation.
- Correctional healthcare: Security restrictions often limit networked device access, making paper a practical fallback.
- Home health: Nurses may complete paper forms in the field when connectivity is unreliable, later reconciling them with a digital system.
- Disaster and field medicine: Emergency deployments rarely have access to cloud-based systems, so paper becomes the default.
Why the Format Matters
The choice between paper and electronic documentation is not just an administrative preference. It shapes how long a nurse spends charting at the end of a shift, how quickly a provider in another department can access a critical lab value, and whether a record holds up in a malpractice review. Understanding the concrete trade-offs, starting with the genuine advantages of paper, gives nurses and practice administrators the foundation they need to make informed decisions.
Advantages of Paper Medical Records
Paper records may feel like a relic in an era of cloud-based platforms and AI-assisted documentation, but for certain practice settings they offer concrete, practical benefits that deserve an honest look.
Lower Upfront Costs
Starting a paper-based charting system requires almost no capital investment. A solo practice can be fully operational with folders, dividers, pre-printed forms, and a filing cabinet. There are no software licenses to renew, no server infrastructure to maintain, and no IT department to budget for. For community clinics, rural practices, or providers just launching a new service, that financial simplicity can be decisive. Even larger facilities that already carry heavy overhead sometimes maintain paper records for specific departments where the cost of a full EMR rollout is hard to justify.
No Dependency on Technology
Every nurse who has worked through a system outage knows the quiet panic that sets in when the EMR goes dark. Paper records do not care about power failures, internet disruptions, or ransomware attacks. During a prolonged system downtime, a facility that relies entirely on electronic records can find itself unable to access medication histories, allergy lists, or prior visit notes. Paper charts remain on the shelf, readable by candlelight if necessary. That kind of resilience is not trivial in disaster-prone regions or in facilities with unreliable infrastructure.
Familiarity, Speed, and Customization
Veteran nurses and providers who trained on paper charting often find it faster for short, routine encounters. There is no login sequence, no drop-down menu to navigate, and no mandatory field blocking the next screen. The documentation follows the clinician's own logic rather than a vendor's workflow assumptions.
Customization is another quiet strength. A clinician can design an intake form, a flow sheet, or a progress note template in an afternoon, with no IT ticket, no vendor approval, and no implementation timeline. If the form does not work, it gets revised just as quickly.
The Tactile Review Factor
Some providers describe a genuine cognitive advantage when reviewing physical charts. Flipping through a paper record allows a provider to absorb the arc of a patient's history in a way that scrolling through discrete EMR fields sometimes does not replicate as naturally. For complex, long-term cases, holding the chart and moving between sections can surface patterns that a screen-based review might fragment across tabs and timestamps. This is not universal, but it is reported often enough among experienced clinicians to merit acknowledgment.
Disadvantages of Paper Medical Records
Medication administration errors occur at rates of 2.8 to 16 percent when nurses rely on paper medication administration records (MARs), a range documented across 18 peer-reviewed studies examining nursing practice in hospitals and long-term care settings.1 This error rate reflects the inherent limitations of paper-based documentation: illegible handwriting, missing signatures, and the inability to trigger automated safety checks at the point of care.
Storage Limitations and Physical Space Costs
Paper charts demand substantial physical infrastructure. Medical practices allocate hundreds of square feet to record rooms, filing cabinets, and off-site archiving. As patient panels grow and retention requirements stretch to seven years or more under state and federal law, the cost of real estate, climate control, and secure storage compounds. Practices in high-rent urban markets face particularly steep overhead, and rural nursing clinics often lack secure off-site facilities altogether, forcing them to convert treatment space into file storage.
Legibility and Medication Error Risk
Handwriting misreads remain a documented source of adverse drug events. Research comparing paper and electronic medication systems found that transitioning from paper charting reduced medication administration errors by 23 percent.2 One hospital using electronic health records for over a decade reduced wrong-dose or unclear-dose errors by 772 cases between 2013 and 2023, demonstrating the preventable harm tied to handwritten orders.3 Even when nurses transcribe orders carefully, the original physician note may be ambiguous: a "1" mistaken for a "7," a decimal point lost in hurried script, or a drug name confused with a sound-alike.
Lack of Interoperability and Care Fragmentation
Paper records cannot be transmitted electronically. When a patient visits a specialist, the primary care office must mail, fax, or hand-deliver a photocopy. Labs send printed results that arrive days late. Pharmacies cannot verify allergy histories in real time. Insurance companies request duplicate charts for prior authorization. Each handoff introduces delay, the risk of lost pages, and the possibility that critical information never reaches the next provider. The result is fragmented care: duplicate tests, missed contraindications, and preventable readmissions.
Scalability Problems and Retrieval Delays
As patient volume climbs, paper systems break down. Retrieval time lengthens when files are misfiled or pulled for billing audits. Duplicate charts proliferate when a nurse cannot locate the original and starts a new folder. In busy emergency departments, a missing chart can delay triage decisions. Practices that serve hundreds of patients per day find that paper workflows cannot keep pace, forcing staff to search bins and shelves instead of focusing on patient care.
Vulnerability to Loss and Irreversible Damage
Paper records have no backup. Fire, flood, mold, vermin, and simple misfiling can destroy decades of patient history in minutes. Theft of charts for identity fraud has been documented, and once a paper file leaves the building, control is lost. Unlike electronic systems with redundant servers and encrypted backups, paper offers no recovery mechanism. When Hurricane Katrina flooded New Orleans hospitals in 2005, entire medical archives were destroyed, leaving thousands of patients without documentation of chronic conditions, medication histories, or surgical records.
Questions to Ask Yourself
Paper Medical Records Vs. EMR: Side-By-Side Comparison
The cost gap between paper and electronic medical records is wider than most practitioners realize, and storage expenses are only one piece of the puzzle. When you factor in retrieval time, error rates, regulatory compliance, and long-term scalability, the differences between these two systems become even more striking.
Storage and Per-Document Costs
Published cost analyses place the per-document storage cost for paper records at roughly $0.045 per document per year, while the equivalent electronic storage cost sits near $0.0002 per document per year.1 That may sound negligible on a per-page basis, but a busy primary care practice can generate tens of thousands of documents annually. Over a decade, the cumulative expense of filing cabinets, off-site storage facilities, and the square footage dedicated to chart rooms adds up quickly. EMR systems require upfront implementation costs and ongoing subscription fees, yet the per-document savings compound as the practice grows.
Retrieval Speed and Accessibility
Paper charts must be physically located, pulled from a shelf or archive, and returned after use. In practices with multiple locations, obtaining a patient's complete history can take hours or even days. Electronic records, by contrast, are retrievable in seconds from any authorized terminal or device. For nurses coordinating care across departments or facilities, immediate access to labs, medication lists, and provider notes can directly influence clinical decisions and patient outcomes.
Error Rates and Legibility
Handwritten entries are a well-documented source of medication errors, misread orders, and incomplete documentation. While EMR systems are not immune to data-entry mistakes, built-in safeguards like allergy alerts, dosage calculators, and mandatory fields reduce the likelihood of critical oversights. Paper records offer no such safety net.
Key Differences at a Glance
- Per-document storage cost: Paper records cost approximately 200 times more per document per year than their electronic counterparts.1
- Retrieval time: Paper charts require manual search and physical transport; EMRs deliver instant access.
- Error reduction: EMRs include clinical decision support tools; paper records rely entirely on human accuracy.
- Scalability: Adding patients to a paper system means more physical space and labor; EMR capacity scales with minimal incremental cost.
- Disaster resilience: Paper records are vulnerable to fire, flooding, and physical deterioration; electronic records can be backed up across multiple secure locations.
What This Means for Your Practice
Total cost-of-ownership comparisons from health IT analysts generally show that EMR systems, despite higher initial investment, become more cost-effective within a few years of implementation for most practice sizes. Solo practitioners may see a longer break-even timeline due to the fixed costs of software licensing, while small group and mid-size clinics tend to recoup their investment more quickly through labor savings and reduced physical storage needs. If your facility still relies on paper charting, understanding these cost and workflow differences is the first step toward evaluating whether a transition, or at least a hybrid approach, makes sense for your team and your patients.
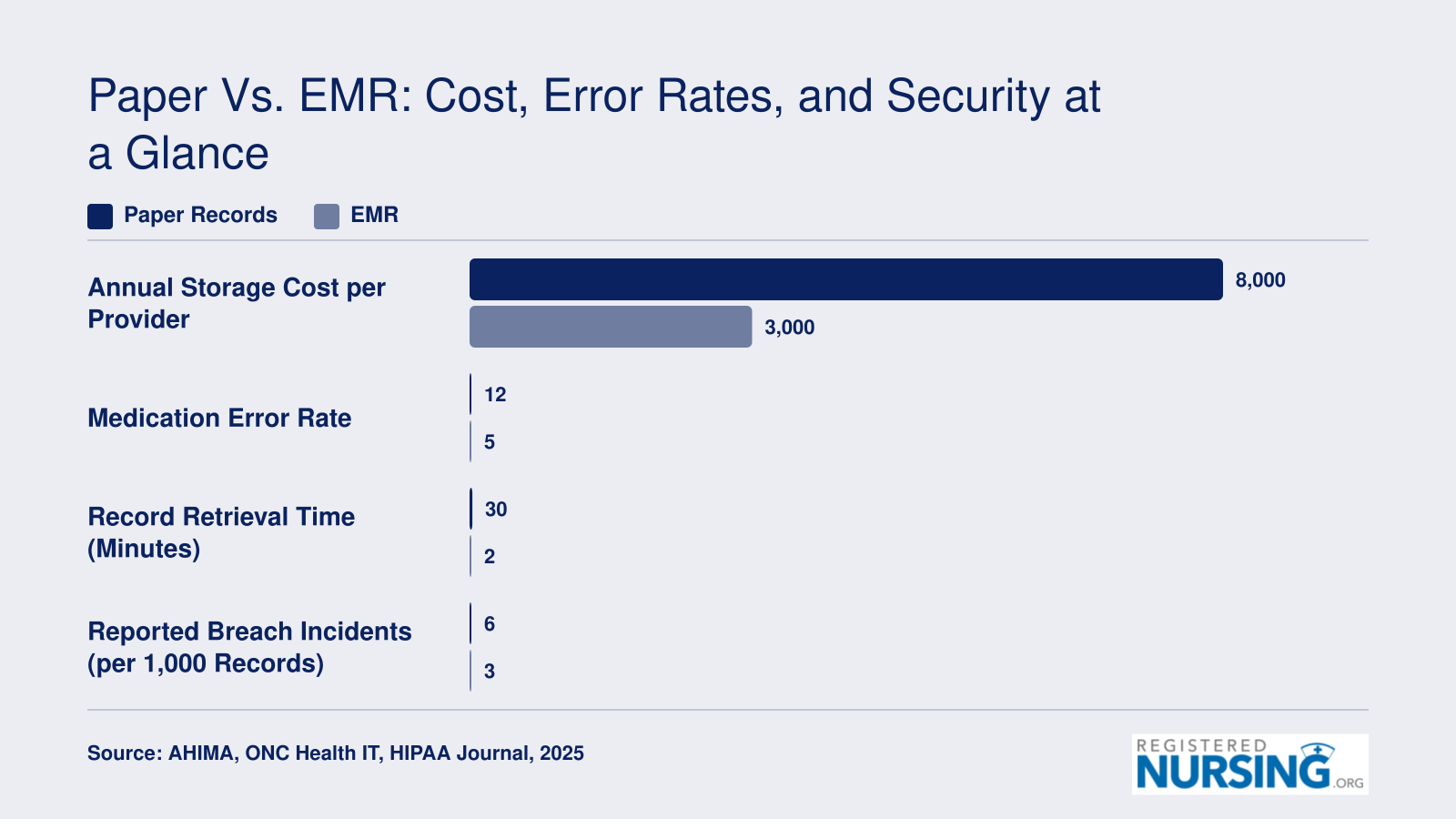
Paper Vs. EMR: Cost, Error Rates, and Security at a Glance
When comparing paper medical records to electronic medical records, the differences in cost, error frequency, and data security become clear at scale. While paper charting may cost less upfront for solo or very small practices, EMR systems tend to deliver lower total cost of ownership as patient volume grows, along with measurable improvements in accuracy and security.
HIPAA Compliance and Legal Considerations for Paper Records
HIPAA applies to protected health information in every form, whether stored on a server or in a manila folder. A common misconception is that paper charts fall outside HIPAA's reach because the Security Rule specifically governs electronic PHI.1 That is only half true. The Privacy Rule still requires reasonable safeguards for paper records, and the penalties for a paper breach are identical to those for a digital one.1
Physical Safeguards and Disposal
For paper charts, HIPAA expects covered entities to prevent unauthorized viewing, access, loss, theft, and improper disposal.1 In practice, this means:
- Storage: Locked file rooms or locked cabinets with restricted access to authorized staff only.
- Access control: Applying the minimum-necessary standard, so employees only pull charts relevant to their role.
- Transport: Sealed envelopes, covered carts, or secure containers when charts move between departments or offices.3
- Disposal: Cross-cut shredding, incineration, or pulping. Tossing intact charts into a dumpster is one of the most frequently cited paper-record violations.
Retention Requirements
HIPAA itself requires covered entities to retain compliance documentation (policies, authorizations, disclosure logs) for six years.2 Actual medical record retention, however, is governed by state law, and the timelines vary considerably:
- California: 7 years after the last date of service, and for minors, until the patient turns 19 (or longer in some cases).2
- Texas: 7 years, with longer periods required for minor patients.2
- New York: 6 years, and until age 22 for records of minors.2
- Florida: 5 years after the last patient contact, with extended timelines for minors.2
Facilities operating across state lines must comply with the longest applicable period.
The Audit Trail Gap
An electronic system logs every user who opens a chart. Paper offers no equivalent. To document access, facilities must maintain manual sign-out sheets or chart-tracking logs, and enforcement is famously inconsistent. Nurses familiar with consent form signing for nurses understand how critical a clear, verifiable paper trail can be: when an OCR investigator asks who viewed a specific record on a specific date, a shrug is not an acceptable answer.
Breach Notification and Penalties
A stolen box of charts from a car trunk, a folder left in a taxi, or records dumped in an unsecured recycling bin all trigger the same breach notification obligations as a ransomware attack: notify affected patients, notify HHS, and if the breach involves 500 or more individuals, notify the media.2 Civil penalties can reach into the millions per violation category per year, regardless of whether the records were paper or electronic. Small practices, in particular, tend to underestimate this exposure.
Related Articles
Security Risks: Paper Records Vs. Electronic Records
Both paper and electronic records carry genuine security risks, but the nature of those risks differs in important ways. Understanding those differences helps nurses and administrators make informed decisions about documentation systems and the safeguards each requires.
How Paper Records Are Compromised
Physical records can be lost, stolen, misfiled, or destroyed without leaving a digital trace. A misplaced chart, an unlocked filing cabinet, or an improperly disposed document can expose patient information just as seriously as a cyberattack. Water damage, fire, and simple human error also threaten physical archives in ways that are difficult to reverse. Once a paper record is gone, recovery depends entirely on whether a duplicate or backup copy exists, and in many facilities, none does.
Unauthorized access is another concern. A staff member or visitor with physical proximity to a records room can view or remove documents without triggering any automatic alert. Unlike electronic systems, paper does not generate access logs, so detecting inappropriate review of a record after the fact is often impossible.
How Electronic Records Are Compromised
Electronic health records face a different threat landscape. Hacking, ransomware, phishing attacks, and insider misuse are among the most common causes of large-scale electronic breaches. When a breach occurs in a digital environment, the number of patients affected can be enormous, because a single compromised database may contain millions of records.
That scale distinguishes electronic breaches from paper ones in a meaningful way. Paper breaches tend to affect a smaller number of records at a time, simply because physical theft or loss has practical limits. Electronic incidents, by contrast, can propagate across entire networks within hours.
Where the Data Points
The HHS Office for Civil Rights maintains a publicly accessible breach portal that logs reported incidents by record type, covering both physical and electronic media. Study findings on Americans' top health questions illustrate how public interest in data privacy and health information security has grown alongside these documented trends. Reviewing that portal, along with annual summaries from organizations like HIMSS and AHIMA, gives a clearer picture of breach frequency and trends over time. Academic databases such as PubMed also publish peer-reviewed analyses that draw on this federal data to compare breach severity across record types.
For any facility evaluating record security, consulting those sources directly, rather than relying on secondhand summaries, provides the most current and defensible foundation for policy decisions. Neither paper nor electronic systems are inherently safe. Each demands specific, deliberate safeguards matched to its particular vulnerabilities.
Illegible handwriting on paper medical records remains a major source of medication errors in healthcare settings. According to research on medication safety practices, handwriting legibility issues contribute to misread drug names, incorrect dosages, and wrong administration routes. These preventable errors underscore why many facilities have moved toward electronic prescribing systems.
How Paper Records Affect Nursing Workflow and Patient Safety
The discussion around nursing documentation has shifted considerably as electronic health records become the standard, yet paper records still influence workflow in many clinical settings. How a nurse documents directly impacts how quickly care is delivered and the likelihood of mistakes. Below, we examine key areas where paper records affect nursing workflow and patient safety.
Time Burdens in Paper-Based Workflows
Manual documentation requires nurses to physically locate and handle patient charts, often walking to a central nursing station or file room. This process can fragment a nurse's schedule and reduce time at the bedside. While precise figures vary, research consistently finds that paper charting extends the time needed to record and retrieve information compared to electronic systems. Nurses may spend a substantial portion of a shift on documentation when using paper, which can delay response to patient needs and contribute to fatigue.
Legibility, Errors, and Safety Risks
Illegible handwriting remains one of the most cited drawbacks of paper records. Misread orders or notes can lead to medication errors, incorrect dosages, or overlooked allergies. Nursing literature frequently points to such documentation breakdowns as a factor in adverse events. In addition, paper forms can be inconsistent, leading to missing data fields or ambiguous notations. Without automated alerts or clinical decision support found in EMRs, the onus falls entirely on the nurse to cross-check information, increasing the risk of oversight.
Accessibility and Continuity of Care
Paper charts exist in one physical location at a time. This limits simultaneous access by multiple providers, slowing interdisciplinary communication. When a chart is missing or misplaced, critical health information may be unavailable at a critical moment, delaying treatment decisions. In contrast to digital systems that allow instant viewing from any approved terminal, paper imposes a sequential, often delayed, flow of information. For nurses coordinating with physicians, pharmacists, and specialists, these delays can interrupt the continuity of care and fragment the care team's shared understanding of a patient's status.
Balancing the Workflow Equation
While some nurses appreciate the tactile simplicity of paper and the ability to quickly jot notes without navigating software, the cumulative effect on workflow efficiency and error potential tilts the balance toward electronic documentation in most care environments. Nevertheless, understanding the impact of paper on nursing practice helps institutions design better workflows, whether they are transitioning to an EMR or maintaining hybrid systems. By recognizing that documentation is not merely a clerical task but a core patient safety activity, nursing leaders can advocate for systems that protect both clinician time and patient outcomes.
Transitioning From Paper to EMR: Hybrid Strategies and Best Practices
Moving from paper charts to an electronic medical record system is a process, not a flip of a switch. Organizations rarely succeed by mandating an overnight change. Instead, most facilities adopt a transition model that balances speed with safety, giving staff time to learn new workflows while preserving continuity of care.
Four Common Transition Models
Facilities typically choose from four approaches. A cold-turkey conversion means setting a go-live date and switching entirely to the EMR, leaving paper behind except for archived records. This requires extensive advance training and carries the highest risk of productivity loss, but it produces the fastest adoption and eliminates duplicate documentation.
A phased rollout by department starts the EMR in one unit such as the emergency department or outpatient clinic, refines workflows, then rolls out to additional departments in waves. This model spreads risk and allows early lessons to inform later phases, but it requires longer project timelines and coordination across paper and electronic systems.
A parallel run operates paper and EMR side by side for a defined period, often 30 to 90 days. Nurses document in both systems during this window, catching EMR errors before abandoning the paper safety net. This approach reduces risk but doubles charting workload and extends the transition period.
A permanent hybrid keeps certain forms on paper indefinitely. For example, surgery consent forms, flow sheets for specific procedures, or inpatient admission packets may remain paper-based while routine orders and progress notes go electronic. This works when scanning these forms into the EMR is simpler than building custom electronic templates.
Scanning and Backfile Decisions
One early decision is whether to digitize existing paper charts or start fresh. Scanning every archived chart is expensive, often $1 to $3 per page, and a single patient record can exceed 100 pages. Many organizations scan only active patient charts for individuals seen within the past two years, then store older paper records offsite or according to state retention rules. Scanning becomes cost-effective when staff frequently retrieve old records or when physical storage costs approach scanning costs.
Staff Training and Productivity Impact
Budget dedicated EMR training time for every nurse, typically 8 to 16 hours of classroom or online modules plus another 8 to 12 hours of hands-on practice. Assign super-users, experienced nurses who receive advanced training and provide floor support during go-live. Plan for temporary productivity drops: nurses often take 20 to 30 percent longer to complete charting during the first three months as they navigate new screens and workflows. Adjust staffing ratios or delay elective procedures during this learning curve.
Common Pitfalls to Avoid
Underestimating data migration costs is a frequent error. Moving patient demographics, allergy lists, medication histories, and problem lists from paper to the EMR requires manual data entry or expensive interface work, and the bill can exceed software licensing costs.
Paper records sometimes vanish during the transition window. Staff leave charts on desks, in exam rooms, or in hallway bins, assuming someone else will scan or file them. Implement strict workflows for every paper document that enters the building after go-live.
Failing to update HIPAA policies for the hybrid environment leaves security gaps. If nurses print EMR notes to carry on rounds or photocopy lab results, those paper printouts require the same safeguards as legacy paper charts. Revise your breach notification plan and document retention schedule to cover electronic and hybrid records.
Pre-Go-Live Checkpoint
Before flipping the switch, confirm you have a signed vendor contract with defined support hours, a documented backup workflow in case the system goes down, written sign-off from nursing leadership that staff training is complete, and an updated HIPAA policy that covers the new record format. Missing any of these invites delays, compliance gaps, or patient safety incidents in the first critical days.
Frequently Asked Questions About Paper Medical Records
Below are answers to some of the most common questions nurses, nursing students, and practice managers ask about paper medical records. Each response draws on points covered earlier in this article.
- What are the disadvantages of paper medical records?
- Paper records are vulnerable to physical damage from fire, flooding, and general wear. They can only be accessed by one person at a time, which slows care coordination. Handwriting legibility issues increase the risk of medication errors, and retrieving a specific chart from a large filing system is time consuming. Storage costs also grow steadily as patient volumes increase, and tracking who accessed a record is far more difficult than with electronic systems.
- What are the advantages of paper medical records over EMR?
- Paper records do not depend on electricity, internet connectivity, or software uptime, making them resilient during power outages and cyberattacks. They require no specialized training to create or read, and there are no software licensing or IT maintenance fees. Many clinicians also find that writing narrative notes by hand encourages more thoughtful, individualized documentation. For very small practices, paper can be a lower cost option in the short term.
- What are the HIPAA requirements for storing paper medical records?
- HIPAA requires that paper records be stored in locked cabinets or rooms with access limited to authorized personnel. Practices must maintain written policies governing who may view patient files, implement sign out logs to track chart movement, and use secure shredding or incineration for disposal. Staff training on privacy procedures is mandatory, and a breach notification process must be in place if records are lost or improperly disclosed.
- How do paper medical records affect patient safety and nursing workflow?
- Nurses working with paper charts often spend significant time locating, pulling, and refiling records. Illegible handwriting can lead to misread orders, incorrect dosages, or missed allergies. Paper systems also lack built in clinical decision support tools, such as drug interaction alerts, that electronic records provide automatically. These workflow inefficiencies can increase the chance of documentation gaps and delay care, particularly during shift changes or patient transfers.
- How do you transition from paper medical records to electronic health records?
- Most organizations use a phased or hybrid approach. Start by digitizing active patient records through scanning, then implement the new EMR system in stages, beginning with scheduling or billing before moving to clinical documentation. Staff training is essential, and running paper and electronic systems in parallel for a transition period helps catch errors. Designating "super users" on each unit can support colleagues during the learning curve.
- Which of the following may be a disadvantage of paper records?
- This is a common multiple choice question on nursing exams. The correct answer typically highlights limited accessibility, because paper charts can only be in one physical location at a time. Other valid disadvantages tested include susceptibility to damage or loss, difficulty auditing access, lack of automated error checks, and high long term storage costs. If you encounter this question, look for the option that addresses retrieval or sharing limitations, as these are the most frequently cited drawbacks in clinical practice.
Is paper charting the right choice for my practice, or am I holding my team back? Paper records offer lower upfront costs and work when the power goes out, but those savings often evaporate under the weight of safety risks and compliance demands. Medication error rates linked to paper MARs range from 2.8 to 16 percent, and retrieval time and legibility issues compound at higher patient volumes.
An EMR delivers stronger audit trails, faster data access, and scalable compliance, though it requires a meaningful investment. For solo or very small practices with low regulatory exposure, paper may still suffice. Larger or busier facilities typically find EMRs pay for themselves in reduced liability and improved workflow. For a deeper look at the electronic side of this comparison, see our companion article on electronic charting pros and cons.