What you’ll learn in this article…
- UNC's 111 student VR pilot used Oculus Quest 2 headsets for mental health clinical hours.
- Research confirms VR improves nursing knowledge and confidence over traditional methods alone.
- Launching a VR classroom for 25 students typically costs $20,000 to $80,000.
Can virtual reality actually replace clinical hours in a nursing program? That question is driving real conversations in nursing schools across the country, and the pressure behind it is not theoretical. Clinical placement shortages contribute to the nursing shortage at every program level, from ADN to DNP, leaving faculty scrambling to secure enough hospital sites to meet accreditation requirements.
In 2024, the University of North Carolina at Chapel Hill ran a pilot that put 111 nursing students in Oculus Quest 2 headsets during a mental health nursing course.1 Students worked through scenarios inside a virtual emergency department exam bay, with modules built by Oxford Medical Simulation, and some of those hours counted toward clinical requirements. The results prompted serious consideration of adding VR permanently to the curriculum.
That pilot is one data point in a broader shift. VR is moving from novelty to infrastructure in nursing education, and how programs adopt it, who can access it, and what regulators will accept are the questions that matter most right now.
What Is Virtual Reality in Nursing Education?
Virtual reality in nursing education represents a spectrum of technologies, each offering different levels of immersion and realism, and each fitting a distinct niche in how students learn clinical skills. Understanding where VR sits on the nursing simulation continuum helps prospective students evaluate whether a program's technology matches their learning preferences and career goals.
Three Main Types of VR Used in Nursing Programs
Nursing programs deploy three primary forms of virtual reality, each with different hardware requirements and learning outcomes:
- Fully immersive VR: Students wear headsets (such as the Oculus Quest 2 used in UNC's pilot) that place them inside a three-dimensional clinical environment where they interact with virtual patients and equipment using hand controllers.
- Desktop or screen-based simulation: Learners navigate clinical scenarios on a computer monitor, clicking through decision trees and patient interactions without wearing a headset, often used for case-based learning and triage practice.
- Game-based learning platforms: These blend VR principles with serious-game design, where students complete missions or challenges (for example, managing a virtual med-surg unit over a shift) to reinforce concepts like delegation and time management.
How VR Differs from Traditional High-Fidelity Manikin Simulation
Virtual reality occupies a distinct place on the simulation spectrum. High-fidelity manikins (physical simulators that breathe, bleed, and respond to interventions) remain the gold standard for hands-on psychomotor skills like IV insertion and chest compressions. VR excels in areas where manikins fall short: simulating complex patient communication, psychiatric presentations, rare emergency scenarios, and entire clinical environments. In UNC's pilot, students entered a virtual emergency department exam bay, practicing mental health assessments in a setting that would be difficult to replicate with a manikin alone. Many programs now layer VR and manikin simulation, using VR for cognitive rehearsal and decision-making, then transitioning to manikins for procedural competency.
What VR Can Simulate in Nursing Education
Virtual reality platforms can recreate patient encounters across the acuity spectrum, from routine assessments to acute decompensation. Students practice in virtual clinical environments (emergency departments, ICUs, home-health visits, psychiatric units) that mirror real-world settings. Critically, VR allows programs to expose learners to rare or high-risk scenarios (anaphylaxis, violent patients, pediatric codes) that students might never encounter during limited clinical rotations, ensuring baseline competency across a wider range of conditions.
VR Across the Nursing Education Pipeline
Virtual reality is not confined to prelicensure BSN degree programs. MSN and DNP students use VR to rehearse advanced assessment techniques and diagnostic reasoning. Nurse practitioner programs deploy VR for complex case management and differential diagnosis practice. Even RN-to-BSN programs integrate VR modules to standardize clinical judgment training for working nurses returning to school. As the technology matures, VR is becoming a common thread across every level of nursing education, from entry-level associate degree programs to doctoral capstone projects.
How Nursing Programs Are Using VR Today: UNC's Pilot and Beyond
One hundred and eleven nursing students at the University of North Carolina at Chapel Hill put on Oculus Quest 2 headsets in 2024 and stepped, virtually, into an emergency department exam bay. The experience was not a video or a slideshow. It was a fully immersive simulation built by Oxford Medical Simulation, placing students in scenarios drawn from mental health nursing practice.
Inside UNC's VR Pilot
The pilot, detailed in a March 2024 report from UNC-Chapel Hill,1 enrolled students in a mental health nursing course. Among them was first-year nursing student Emma Brown, whose cohort used the VR modules to fulfill a portion of their required clinical hours. That detail matters: replacing or supplementing real-world placement time with structured virtual encounters signals a meaningful shift in how programs can meet accreditation and hour requirements when clinical sites are scarce.
The pilot's immediate goal is assessment. Faculty are using student performance and feedback data to decide whether VR becomes a permanent fixture in the curriculum rather than an experiment. That measured approach is worth noting for students evaluating programs. Schools that pilot and then evaluate, rather than simply adopting technology for its own sake, tend to integrate it more thoughtfully.
Why UNC's Model Is Worth Watching
What makes the UNC approach a useful reference point for other programs is its structure. Students encounter the same ED exam bay scenario under the same conditions, which removes the variability that often frustrates clinical learning. One student may spend a hospital rotation observing; another may manage five patient interactions. VR standardizes that experience, ensuring everyone practices the same mental health nursing competencies before entering a live clinical environment.
For nursing education broadly, the shortage of clinical placement sites is a persistent obstacle across ADN, BSN, and nursing degree programs alike. Standardized VR modules offer a scalable path around that bottleneck, particularly for specialized areas like psychiatric and mental health nursing where placements are especially limited.
VR Use Cases Beyond Mental Health
UNC's pilot focuses on one specialty, but programs across the country are applying VR to a wider range of clinical scenarios. Common applications now include:
- Pediatric emergencies: Students practice rapid assessment and intervention in high-stakes situations that would be difficult to replicate safely in simulation labs.
- Medication administration: VR environments walk students through dosage calculations, draw-up technique, and patient verification in a consequence-free setting.
- Interprofessional communication: Some modules place nursing students alongside virtual physicians, pharmacists, and social workers, building the team communication skills that are tested in every real clinical setting.
Taken together, these use cases show that VR is not a niche tool for one course or one program level. It is becoming a flexible instructional layer that can support students from their first clinical skills course through advanced practice preparation.
Questions to Ask Yourself
What the Research Says: Is VR Effective in Nursing Education?
The research is clear enough to act on: virtual reality consistently improves nursing students' knowledge, skills, and confidence compared to traditional instruction alone, even if the evidence base is still maturing.
What the Numbers Show
Several meta-analyses and systematic reviews published between 2023 and 2025 have now pooled results across dozens of individual studies, giving educators and students a more reliable picture than any single trial could provide. One 2023 meta-analysis found a large effect on knowledge acquisition, with a standardized mean difference of roughly 0.97, meaning VR-trained students scored substantially higher on knowledge assessments than comparison groups.1 The same review found a moderate effect on clinical skills and skill retention, both around 0.52, and a notably large effect on student satisfaction, with a standardized mean difference exceeding 1.0.1
A 2024 review that pooled data from 26 studies and more than 1,800 participants found similarly encouraging results.2 Performance outcomes showed a mean difference of about 1.13, while student satisfaction scores improved by roughly 0.82. Self-efficacy, meaning students' belief in their own ability to perform clinical tasks, showed a moderate benefit ranging from 0.5 to 0.7 across that review's outcomes. A separate 2024 analysis specifically measuring nursing competency reported a Hedges' g of 0.88, which falls in the large-effect range.5
A 2025 systematic review broke outcomes into more granular categories and found moderate effects across cognitive learning (0.33), psychomotor or hands-on skill development (0.49), and self-efficacy (0.38).3 These numbers are somewhat smaller than earlier reviews, which likely reflects stricter inclusion criteria and a broader mix of VR types, from fully immersive headset experiences to more basic 360-degree video platforms.
Where the Evidence Is Strongest and Where It Falls Short
Across reviews, VR shows its most consistent advantage in two areas: boosting students' confidence before clinical placements, and delivering standardized, repeatable scenarios that traditional simulation cannot always guarantee. Mental health nursing, emergency care, and procedural skills training have emerged as particularly well-studied applications. One 2024 meta-analysis found a skill effect size of 0.682, suggesting hands-on competency gains are among the most robust outcomes reported.4
The honest caveat is that most underlying studies are small, short in duration, and vary considerably in the type of VR technology used. Long-term skill retention beyond a few weeks, real-world patient safety outcomes, and the comparative effectiveness of VR against high-fidelity mannequin simulation remain areas where the literature is thin. Researchers have also noted that publication bias, where studies with positive results are more likely to be published, may inflate some of the effect sizes seen in meta-analyses.
The Bottom Line for Students and Programs
The cumulative evidence, drawn from thousands of nursing students across multiple countries, is strong enough to support VR as a meaningful supplement to clinical education. It is not yet strong enough to conclude that VR can fully replace traditional clinical hours or hands-on simulation for every learning objective. Programs adopting VR today are making a well-grounded decision, and those that also keep pace with broader AI advances shaping nursing practice will be best positioned as the long-term evidence base continues to grow.
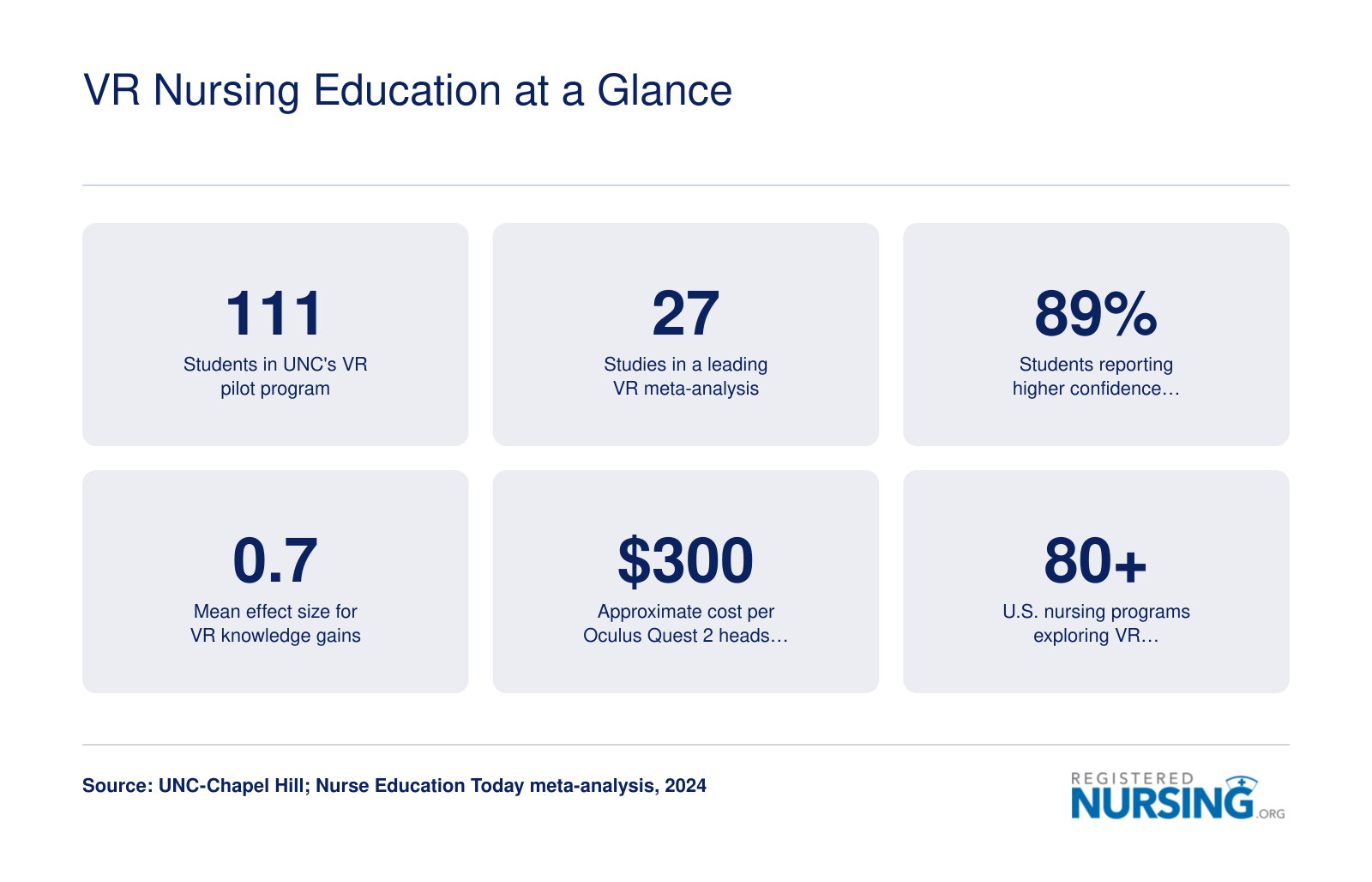
VR Nursing Education at a Glance
Virtual reality is gaining momentum across nursing programs at every level. Here are some of the key numbers shaping the conversation around VR's role in clinical training and education.
Top VR Platforms Used in Nursing Programs
Oxford Medical Simulation: The Platform That Powers UNC's Pilot
The University of North Carolina at Chapel Hill selected Oxford Medical Simulation (OMS) for its virtual reality pilot involving 111 nursing students in a mental health course.1 OMS offers both fully immersive VR headset experiences and screen-based simulations, giving programs flexibility depending on their hardware budget and physical space constraints. Nursing students in the UNC pilot used Oculus Quest 2 headsets to enter a simulated emergency department exam bay, aligning with OMS's broad library of clinical scenarios covering nursing fundamentals, acute care, med-surg, interprofessional practice, and patient assessment.2
Key Features and Technical Requirements
OMS supports multiple delivery modes. For the most immersive experience, students wear a Meta Quest series headset. The platform also runs on PC-tethered VR setups requiring Windows 10, an NVIDIA GTX 1080 or RTX 2070 graphics card, an Intel i7 processor, and 16 GB of RAM. Screen-based simulations need less horsepower: an Intel i5 and 8 GB of RAM suffice.3 This tiered approach allows programs to expand VR access without equipping every seat with a headset. OMS's scenario library goes beyond single-patient encounters to include multi-patient and interprofessional simulations, mirroring the complexity of real clinical environments.
Pricing and Institutional Adoption
Oxford Medical Simulation uses a flexible pricing model that includes pay-per-use options, tiered institutional licenses, and library pricing.4 Exact costs are available only by contacting the vendor, but the structure accommodates both small pilot programs and large-scale deployments. OMS has been adopted by Oxford University and numerous academic and health system partners in the U.S. and U.K., particularly through its OMS Nursing product designed specifically for prelicensure and graduate nursing education.1 The UNC pilot exemplified how a single-semester partnership can help a school evaluate whether to integrate VR permanently into its curriculum.
Other Platforms on the Nursing Education Landscape
While Oxford Medical Simulation is a prominent choice, several other platforms are gaining traction. SimX, VRpatients, and Shadow Health also offer virtual simulation environments, though their features, hardware requirements, and pricing vary. Program directors typically compare scenario breadth, ease of faculty customization, integration with EHR solutions for nurses, and total cost of ownership. Screen-based options from these vendors can be more accessible for schools that are not yet ready to invest in headset fleets.
What to Look For When Evaluating a VR Platform
When selecting a VR solution, nursing programs should consider clinical scenario relevance to their curriculum, hardware and IT support requirements, and the availability of analytics to track student performance. The ability to fulfill a portion of clinical hours, as seen in the UNC pilot, also depends on regulatory acceptance by state boards of nursing. Institutions should also examine how each platform handles updates to clinical guidelines and whether faculty can build or modify scenarios. Requesting a pilot or demo, as UNC did, remains the most reliable way to assess whether a platform will meet a program's specific educational goals. Program leaders evaluating technology tools may also find it useful to read NCLEX-RN pass rate data when evaluating nursing schools to connect simulation investments to measurable outcomes.
Cost, Infrastructure, and Accessibility Considerations
$20,000 to $80,000 represents the typical range nursing programs spend to establish a VR classroom equipped for 20 to 25 students, according to institutional deployment data from 2024 through 2026.1 This investment encompasses hardware, software licensing, IT infrastructure upgrades, and faculty preparation time. Understanding these costs helps prospective students evaluate program resources and helps educators plan realistic implementation timelines.
Hardware Costs: From Headsets to Workstations
The most visible expense is the VR headset itself. Consumer-grade Meta Quest 2 headsets retail between $299 and $479, but educational deployments typically run closer to $600 per unit once device management software and protective cases are factored in.2 Enterprise versions of the Quest 2, which include enhanced security features and centralized administration tools, cost approximately $800 upfront plus $180 annually for support.3 The newer Meta Quest 3 ranges from $500 to $600, while high-fidelity systems like the HTC Vive Pro run between $900 and $1,200 per headset.1 For programs using PC-tethered VR rather than standalone headsets, a VR-ready computer adds $1,200 to $2,000 per station.1 When calculated per student seat, fully installed costs typically land between $800 and $4,000 depending on the level of immersion and redundancy built into the system.
Software Licensing and Platform Fees
Beyond hardware, nursing programs pay annual licensing fees to access clinical simulation content. Mid-sized labs typically budget $2,000 to $10,000 per year for VR nursing software, while larger programs with multiple cohorts or specialty tracks may spend $5,000 to $15,000 annually.4 These fees cover scenario libraries, software updates, performance analytics dashboards, and sometimes faculty training modules.
Some vendors offer tiered pricing based on student enrollment or concurrent user limits, which can help smaller programs manage costs. Grant funding, vendor partnerships, and tuition reallocation are common strategies institutions use to absorb these expenses without passing them directly to students.
Faculty Training and Workload Impact
Implementing VR requires faculty to learn new technical skills and pedagogical approaches. Initial training sessions can consume 10 to 20 hours per instructor, with ongoing time needed for scenario customization and troubleshooting. However, once faculty become proficient, VR can reduce some instructional burdens by providing standardized, repeatable patient encounters that require less real-time supervision than traditional simulation labs.
Programs should budget not only dollars but also protected faculty development time during the first year of adoption. Without adequate preparation, VR investments risk underutilization. Students working while in nursing school may find VR's flexible, on-demand practice format especially valuable when scheduling clinical hours around work commitments.
Equity and Accessibility Concerns
Not all students experience VR equally. Motion sickness, sometimes called cybersickness, affects a subset of users and can limit participation without accommodations such as reduced session lengths or alternative viewing modes. Students with certain visual impairments or vestibular conditions may require modified scenarios or non-VR alternatives to meet learning objectives.
Underfunded programs face a steeper path to adoption. A $40,000 classroom setup may be manageable for a well-resourced university but prohibitive for community colleges serving first-generation nursing students. This disparity raises questions about whether VR narrows or widens the digital divide in nursing education, much as advantages and disadvantages of electronic health records have long separated well-resourced systems from underfunded ones. Students at institutions without VR resources may graduate with less exposure to immersive clinical training, potentially affecting their competitiveness in the job market.
Some vendors and grant programs specifically target underserved institutions to address this gap, but progress remains uneven. Prospective students should ask programs directly about VR availability, accommodation policies, and how costs are distributed across tuition and fees.
At first glance, virtual reality looks affordable: standalone headsets now cost less than $500 per unit. But the true expense lies in software licensing fees, dedicated IT support, and extensive faculty training, which can quickly overwhelm tight budgets. Consequently, well-resourced nursing programs are moving ahead with immersive simulations, while others risk falling behind in clinical training quality. This disparity threatens to create two tiers of training.
Accreditation, Clinical Hours, and Regulatory Considerations
The question of whether hours spent in a VR headset can substitute for time on a hospital floor sits at the center of an active regulatory conversation, and the answer in 2026 is more nuanced than a simple yes or no. Programs, accreditors, and state boards are still working out how immersive simulation fits into the clinical hour equation, which is exactly why pilots like UNC's matter beyond their campus.
How CCNE and ACEN View Simulation Hours
Neither the Commission on Collegiate Nursing Education (CCNE) nor the Accreditation Commission for Education in Nursing (ACEN) currently imposes a specific cap on how many simulation hours can count toward clinical requirements.1 CCNE's 2021 Standards, which remain in effect through 2026, explicitly recognize simulation as a teaching-learning practice and treat VR as part of the broader category of virtual and laboratory environments.2 ACEN similarly recognizes simulation as a legitimate type of clinical learning experience and treats VR as one modality within that umbrella.3
Revised CCNE standards were approved in December 2025 and take effect January 1, 2027, so programs should watch for updated procedural guidance as that transition approaches.2 In the meantime, accreditors expect programs to document total clinical hours, the proportion delivered via simulation, and evidence of state regulatory compliance.1
Faculty Oversight, Debriefing, and Outcome Evidence
Both accreditors emphasize how simulation is delivered, not just how much of it happens. ACEN expects faculty to be trained in simulation pedagogy and requires that experiences be structured, debriefed, and formally evaluated.3 CCNE calls for systematic evaluation of simulation, including VR, with outcome evidence such as NCLEX-RN exam preparation outcomes and clinical evaluations.1 ACEN adds employer evaluations to that evidence base. Programs are also expected to validate that VR activities are equivalent to traditional experiences for developing the targeted competencies.1 In practice, this means a VR mental health scenario cannot simply replace a psychiatric final clinical rotation in nursing school without documented pedagogical rigor behind it.
State Boards and the VR-Specific Question
State boards of nursing add another layer, and their rules vary considerably. Following the landmark NCSBN National Simulation Study, many states permit up to 50 percent of clinical hours to be completed via simulation, while others set stricter ceilings or require board approval for higher percentages. Students should check their specific state's regulations before assuming VR hours will count.
One important distinction: accreditors and boards may treat screen-based virtual simulation differently from immersive headset VR. Because immersive VR is newer, formal guidance specifically addressing it is still emerging. UNC's pilot was designed in part to test whether VR-fulfilled clinical hours could be formally incorporated into the curriculum, a signal that this is an active policy frontier rather than settled ground. For students considering choosing an online nursing program, understanding how your program documents and validates simulation hours is one of the most important questions to ask during the admissions process.
Tips for Nursing Students to Maximize VR Learning
Students who treat virtual reality sessions as casual tech demos tend to get far less out of them than students who show up prepared. Approaching every VR simulation with the same intention you bring to a hospital clinical makes a measurable difference in retention, clinical reasoning, and confidence when the real moment arrives.
Prepare Before You Put on the Headset
A few minutes of preparation before each session pays dividends. Read the patient scenario overview, review relevant pharmacology or assessment criteria, and set a clear learning goal for that session. Many platforms let you review case details in a standard screen view before you enter the immersive environment, so use that window. When you step into the virtual exam bay, your brain will engage more deeply if it already has a framework to hang new information on.
Debrief Honestly After Every Session
The learning does not end when you take the headset off. Most VR platforms used in nursing programs include built-in performance data: time on task, decision points, errors flagged, and areas reviewed. Look at those results the way you would review a graded skills check-off. Ask yourself what clinical reasoning steps you skipped, where you hesitated, and what you would change on a second attempt. Writing a brief three-sentence reflection immediately after the session, before you move on with your day, reinforces the experience far more than letting it sit. Students who are newer to self-directed learning can find guidance on navigating nursing school expectations in resources covering during and after RN school.
Use VR as a Bridge Between Classroom and Clinical
VR works best as a rehearsal space, not a replacement for human clinical experience. If you have a clinical rotation coming up in a pediatric unit or an emergency setting, look for matching VR modules to run through beforehand. Equally useful: after a real clinical shift, revisit a related VR scenario to reinforce what you observed. This back-and-forth approach helps consolidate skills and surface gaps you might not notice in the middle of a busy unit. The same principle applies as you advance your education, since AI in nursing is reshaping how both classroom and clinical competencies are assessed across RN, BSN, MSN, and DNP programs.
Speak Up About Accessibility Needs Early
Motion sickness, photosensitivity, and certain visual impairments can make standard headset use uncomfortable or impossible. These are documented, manageable challenges, and nursing programs are increasingly prepared to offer alternatives such as screen-based simulation or modified session lengths. Some students with social anxiety or sensory sensitivities may also find it helpful to review strategies shared for introverted nursing student tips before their first immersive session. The key is telling your faculty or simulation coordinator before the scheduled lab, not during it. Early communication gives programs time to arrange accommodations and ensures you receive the full educational benefit of the module in a format that works for you.
The Future of VR in Nursing Education
Nursing education has always adapted to new tools, from mannequin simulators to high-fidelity labs. The next wave of change is already taking shape, and the pace is accelerating in ways that matter for anyone entering or advancing in the profession today.
AI-Driven Scenarios That Learn With You
The most consequential near-term development is the integration of artificial intelligence into VR simulations. Rather than delivering a fixed script, AI in nursing modules adjust difficulty, patient acuity, and clinical complexity in real time based on how a student performs. If you move too quickly through an assessment or miss a deteriorating vital sign, the scenario responds. If you consistently demonstrate strong prioritization, the system escalates the challenge. This kind of adaptive learning mirrors what experienced preceptors do intuitively, except it scales to an entire cohort simultaneously and provides consistent feedback regardless of clinical site or instructor availability.
Haptic Feedback: The Missing Sense
Current VR systems are largely visual and auditory. The next frontier is touch. Haptic feedback devices in active development could allow students to feel resistance when inserting an IV catheter, detect a bounding or thready pulse, or sense differences in skin temperature during a circulatory assessment. These sensations are difficult to replicate in mannequin labs and nearly impossible to standardize across clinical placements. Haptic integration is still emerging and not yet widely available in nursing programs, but prototypes are advancing and cost curves for the hardware are expected to follow the same downward trajectory that made headsets like the Oculus Quest affordable.
Expansion Into Advanced Practice and Interprofessional Training
VR is moving beyond prelicensure programs. Advanced practice APRN careers in nurse practitioner, DNP, and other advanced-practice curricula are beginning to incorporate immersive case-based scenarios that match the complexity those roles demand. Equally significant is the growth of interprofessional education environments, where nursing students train inside shared virtual spaces alongside medical and pharmacy students. Coordinating a sepsis response or navigating a difficult family conversation with other disciplines present builds the communication and teamwork skills that clinical rotations often provide inconsistently.
A Realistic Timeline
VR will not replace bedside clinical training, and no credible voice in nursing education is arguing that it should. The tactile, relational, and unpredictable dimensions of real patient care remain essential. What VR will increasingly do is fill gaps, standardize foundational skill-building, extend access to students in underserved regions, and grow into a recognized component of accredited programs as regulatory bodies refine their policies. Costs are falling, the evidence base is building, and the programs piloting these tools today are laying the groundwork for what mainstream nursing education will look like within the next decade. For those weighing the long-term value of advanced credentials, understanding why a DNP degree is becoming essential offers useful context for where the profession is heading.
Frequently Asked Questions About VR in Nursing Education
Below are some of the most common questions prospective and current nursing students ask about virtual reality in nursing education. Each answer draws on current evidence and real program examples to give you a practical, honest picture of what VR means for your training.
- What are the benefits of virtual simulation in nursing education?
- Virtual simulation lets students practice high-stakes scenarios, including mental health crises, medication errors, and emergency triage, in a safe, repeatable environment. Students can build clinical judgment, communication skills, and confidence before entering a live patient setting. Programs also benefit from standardized experiences, meaning every learner encounters the same scenario and receives consistent feedback regardless of clinical site availability.
- How effective is virtual reality in nursing education based on meta-analysis findings?
- Multiple systematic reviews and meta-analyses published through 2025 indicate that VR-based simulation produces knowledge and skill gains comparable to, and in some cases exceeding, traditional simulation methods. VR appears especially effective for procedural skills, clinical decision-making, and empathy development. UNC Chapel Hill's 2024 pilot with 111 mental health nursing students reinforced these findings, showing that immersive VR modules helped learners meet clinical competencies while fulfilling a portion of required hours.
- How much does it cost to implement VR in a nursing program?
- Costs vary widely depending on scale. A single consumer-grade headset such as the Meta Quest series may run a few hundred dollars, while institution-wide rollouts with licensed clinical content from platforms like Oxford Medical Simulation can reach tens of thousands of dollars annually. However, per-student costs have been falling as hardware prices drop and subscription models replace one-time licensing fees. Smaller programs can start with a modest headset lab and expand over time. Nursing technology tools, including VR, are increasingly discussed alongside AI in nursing, as both reshape how future nurses learn and practice.
- Can VR clinical hours replace traditional clinical hours in nursing school?
- In most states, VR hours can supplement but not fully replace traditional clinical rotations. Some state boards of nursing and accrediting bodies now allow a defined percentage of clinical time to be completed through simulation, including VR. UNC's pilot, for example, allowed students to fulfill some clinical hours through VR training in mental health nursing. Students should check their state board's rules and their program's accreditation standards, because policies differ significantly. This matters whether you are enrolled in online RN to BSN programs or a campus-based MSN track, as simulation policies vary by program type and state.
- What VR platforms are used in nursing education programs?
- Several platforms serve the nursing education market as of 2026. Oxford Medical Simulation, which powered UNC's pilot program using Oculus Quest 2 headsets, offers scenario-based modules across specialties. Other widely adopted platforms include UbiSim, which focuses on immersive clinical decision-making, and platforms from Laerdal and Shadow Health that blend VR with existing simulation infrastructure. Programs typically choose based on specialty focus, accreditation alignment, and budget.
- What challenges do nursing students face when using VR simulations?
- The most commonly reported challenges include motion sickness or discomfort during extended headset use, a learning curve with the hardware and software controls, and the absence of tactile feedback that comes with practicing on a real manikin or patient. Access can also be a barrier: not all students have equal opportunity to use VR equipment outside scheduled lab times, especially in under-resourced programs. Faculty training and ongoing technical support remain important factors in a successful VR rollout. These access challenges are worth weighing as you consider accelerated ADN programs or other pathways where clinical hour requirements and available resources can differ considerably.
Virtual reality is no longer an experiment; the evidence shows it improves clinical reasoning, skills, and confidence compared to lecture alone, and it is increasingly within reach for nursing programs as hardware prices drop. However, not all VR hours count equally toward licensure requirements, and policies vary by state and program. The most important step you can take right now is to contact your program's simulation coordinator and ask two direct questions: what VR tools are available to you, and exactly how those hours will be credited toward your clinical requirements. If you want to stay ahead of how these changes intersect with broader shifts in the field, exploring emerging nursing specialties can help you anticipate where immersive training will matter most in your career. Knowing the answers puts you in control of your learning path.