What you’ll learn in this article…
- Set specific goals with your mentor during the very first meeting.
- Nursing students say gradual independence matters more than passive shadowing.
- Strong clinical mentorship correlates with higher NCLEX pass rates and starting salaries.
Clinical rotations account for roughly half of most nursing program curricula, yet few schools teach students how to maximize the relationship that determines whether those hours translate into genuine competence. Your clinical mentor is the bridge between classroom theory and bedside practice, the person who watches you draw your first blood, manage your first critical patient, and recover from your first mistake.
Most students arrive at their first rotation without a framework for working with a mentor effectively. They observe, assist, and hope for feedback that may never come unless they know how to ask for it. The difference between a transformative clinical experience and a forgettable one often comes down to online nursing program considerations and goal-setting skills that nobody explicitly teaches. Whether you are pursuing an accelerated ADN program or a doctoral track, the fundamentals of building a productive mentor relationship remain the same.
What Is a Clinical Mentor in Nursing School?
A clinical mentor is an experienced nurse who provides ongoing guidance, supervision, and professional development support to nursing students in the practice setting.1 Unlike a guest lecturer who teaches a single skill or a staff nurse who happens to answer a question, a clinical mentor commits to the student over time. That relationship typically unfolds across weeks or months, giving both people the chance to build trust, identify growth areas, and track progress in a meaningful way.
The term itself is used in different ways across U.S. nursing programs. Some programs call this person a preceptor, a clinical instructor, or a faculty mentor.2 There is no single universally adopted definition from one governing body, which means the title and structure can vary depending on your school and clinical site. What stays consistent is the core purpose: connecting you, the student, to the realities of bedside practice in a supported and structured way.
Core Responsibilities of a Clinical Mentor
At the heart of the role is a set of responsibilities that go well beyond showing you where the supply room is. A clinical mentor is expected to:
- Facilitate learning: Help you meet the specific objectives your program has outlined for each clinical rotation.
- Supervise in the moment: Maintain oversight while you perform assessments, administer medications, or manage patient interactions.
- Assess your performance: Evaluate your clinical competence against defined outcomes, then communicate where you stand honestly and constructively.
- Model professional behavior: Demonstrate what safe, person-centered care actually looks like when the textbook gives way to a real patient in front of you.3
- Support your reflection: Create space for you to process what happened during a shift, build confidence, and develop your professional identity.
Formal and Informal Mentorship
Mentorship in nursing school can be arranged two ways. Formal mentorship is program-assigned: your school or clinical site designates a nurse to work alongside you, with agreed-upon goals and evaluation checkpoints built in. Informal mentorship happens organically. A nurse on the unit takes a genuine interest in your development, invites you into complex situations, and offers guidance without a formal contract behind it.
Both forms carry real value. These dynamics often come into sharpest focus during your final clinical rotation in nursing school, when the stakes are highest and the mentor relationship is tested most directly. The American Association of Colleges of Nursing describes mentorship as a formalized process in which a more knowledgeable individual provides a supportive role, encourages reflection and learning, and helps the learner grow professionally and personally.2 Even when the arrangement is informal, those same qualities mark the difference between a mentor who shapes your career and a supervisor who simply signs off on your hours.
Clinical Mentor Vs. Preceptor Vs. Clinical Instructor: Key Differences
What is the difference between a clinical mentor, preceptor, and clinical instructor in nursing school? These three roles often overlap in practice, which creates confusion for students trying to understand who does what during clinical rotations. Each serves a distinct purpose in your professional development, and knowing the differences helps you engage with each relationship more effectively.
Clinical Instructor: The Faculty Authority
Your clinical instructor is a faculty member employed by your nursing program. This person oversees a group of students on the clinical floor, integrates theoretical concepts with hands-on practice, and carries ultimate academic accountability.1 Clinical instructors hold formal evaluation authority for both clinical performance and course grades. They determine whether you pass or fail clinical courses and are responsible for documenting your progression through the program. The relationship typically lasts the length of a course or academic term.
Preceptor: Your One-on-One Clinical Teacher
A preceptor is a licensed nurse, often a staff nurse at the clinical site, assigned to work with you one-on-one during a specific rotation. According to NCSBN Model Rules, preceptors focus on clinical teaching, supervision, and skill acquisition during direct patient care.2 They are required to evaluate your clinical performance and formally report their observations to faculty or the program. However, preceptors typically do not have final authority over your academic standing.3 Their input informs decisions made by clinical instructors. Preceptor relationships are time-limited, usually lasting weeks to months depending on the rotation structure. For a closer look at what makes this role work well, how to be an effective preceptor offers practical guidance for both students and clinicians.
Clinical Mentor: The Long-Term Guide
A clinical mentor is an experienced nurse who supports your broader career development, professional growth, and reflective practice.4 Unlike preceptors and clinical instructors, mentors usually have no mandated formal evaluation role and no grading or academic progression authority. The mentor relationship can extend months or even years, often continuing well beyond graduation. Mentors help you navigate the transition from student to practicing nurse, offer career guidance, and provide a safe space for questions that feel too basic to ask in graded settings.
Quick Comparison Across Key Dimensions
- Formal authority: Clinical instructors hold the most, preceptors report to them, mentors typically have none.
- Evaluation role: Clinical instructors assign grades, preceptors provide formal clinical evaluations, mentors offer informal feedback.
- Duration: Instructors stay for a term, preceptors for a rotation, mentors potentially for years.
- Setting: Instructors may rotate among students, preceptors work beside you at the bedside, mentors may connect outside the clinical environment.
- Relationship type: Instructors and preceptors fulfill institutional requirements, while mentor relationships are often voluntary and personally chosen.
Understanding these distinctions allows you to approach each person with appropriate expectations and make the most of what each relationship offers. If you are still weighing which nursing degree path best fits your goals, that broader context will also shape the clinical structure you encounter along the way.
How Clinical Mentorship Works Across BSN, MSN, and DNP Programs
Choosing between BSN, MSN, or DNP often involves weighing immediate licensure against advanced practice roles, but the mentorship you'll receive varies significantly by program level. Some paths build mentorship into the curriculum, while others leave it largely to chance.
BSN Programs: Clinical Instructors and Emerging Mentorship
At the bachelor's level, clinical training is typically led by faculty instructors who oversee groups of students, often with support from staff nurse preceptors. Formal, one-on-one mentorship is not a standardized requirement; it appears as an optional element that programs are increasingly encouraged to offer. No national minimum for clinical hours exists, so experiences can differ widely.1 If your BSN program does not formally assign a mentor, proactive students can still seek out experienced nurses on their rotations to fill that role.
MSN and APRN Tracks: Precepted Hours as a Requirement
For master's-entry advanced practice programs, mentorship becomes mandatory. The AACN Essentials (2021) set a benchmark of at least 500 direct-care hours for APRN MSN students,2 while CCNE-accredited NP tracks require 500 hours3 and ACEN-accredited master's NP options may call for 750 hours.1 These hours are completed under a qualified preceptor, often an APRN or physician, whose credentials are reviewed by the accrediting body. Even for non-APRN MSN specializations such as education or leadership, a minimum of 500 practice hours is standard, with mentorship embedded in the experience.2 Direct entry MSN programs offer an accelerated path to these precepted hours for students entering from outside nursing.
DNP Programs: The Most Formalized Mentorship Model
Doctoral-level nursing education takes mentorship the furthest. Best Doctor of Nursing Practice programs typically require DNP APRN students to complete 1,000 practice hours (per CCNE 2024 standards and ACEN 2025 options)31 with a faculty-approved preceptor or mentor. Non-APRN DNP pathways also require substantial hours, ranging from 500 to 1,000 depending on the accreditor.1 At this stage, mentorship is deeply integrated into the curriculum and often involves a long-term, collaborative relationship that shapes the student's scholarly project and clinical expertise.
RN-to-BSN: Mentorship in Capstone and Community Health
RN-to-BSN programs generally have fewer required clinical hours, as students are already licensed. However, mentorship still proves valuable during community health rotations or capstone projects. While not formally mandated by accreditors, many programs encourage students to partner with a mentor who can guide them through population-focused practice or leadership initiatives. Choosing the right capstone focus is a meaningful early step, and guidance on choosing the perfect RN capstone project can help you align that work with your long-term goals.
Required or Recommended? Ask Your Program Coordinator
Whether mentorship is explicitly required or simply recommended varies by accrediting body, program, and even specialty track. The best way to know what to expect is to ask your program coordinator directly: What is the structure for precepted hours? How are mentors selected and vetted? Does the program offer formal mentorship pairings? Clarifying this early ensures you can maximize the mentoring relationship and meet all clinical hour expectations confidently.
Questions to Ask Yourself
How to Choose or Request a Clinical Mentor
Some nursing students interview potential mentors and negotiate placement preferences, while others arrive on day one to meet a randomly assigned preceptor they cannot change. The gap between those two experiences shapes how much agency you can exercise in building a strong mentorship relationship.
The Reality: Many Students Cannot Choose
Most nursing programs assign clinical mentors or preceptors based on availability, unit capacity, and scheduling logistics rather than student preference. In a recent Reddit discussion, one critical care float pool nurse noted that the nursing student assigned to them had been randomly placed and was not permitted to request a specific hospital or unit.1 If you find yourself in this situation, you are not alone. Assignment-based placement is the norm at many BSN, ADN, and nursing degree programs, and your task shifts from choosing a mentor to making the most of the one you are given.
When You Do Have a Say
If your program allows input, prioritize these qualities when requesting or vetting a potential clinical mentor:
- Specialty alignment: Look for a mentor whose unit and patient population match your career interests. If you are aiming for emergency nursing, a mentor in the ED will expose you to relevant workflows and decision-making patterns.
- Teaching reputation: Ask upperclassmen, clinical coordinators, and unit staff which nurses are known for taking time to explain rationale, answer questions, and encourage hands-on practice.
- Communication style: Seek out mentors who provide structured, timely feedback rather than vague or delayed comments. A mentor who debriefs after each shift will accelerate your growth more than one who saves all feedback for the final evaluation.
- Consistent presence: Multiple nursing students report wishing their preceptor had not ditched them during shifts.1 A mentor who stays engaged, observes your practice, and gradually increases your independence is far more valuable than one who disappears or treats you as an extra pair of hands. The power of mentoring in nursing is well documented, and consistent presence is central to that research.
What to Do When the Fit Is Poor
If your assigned mentor is frequently absent, dismissive, or unable to provide the learning environment you need, address the issue with your clinical coordinator or faculty liaison early in the rotation. Frame the conversation around learning-style mismatch rather than personal complaint. For example, you might say, "I am looking for more opportunities to practice independently and receive real-time feedback. Can we discuss strategies to improve that, or would a different placement better support my learning goals?" Early intervention prevents weeks of lost learning and demonstrates professional self-advocacy. If speaking up feels difficult, resources on navigating nursing school as a shy nursing student offer practical strategies for voicing your needs in high-stakes clinical settings.
Setting Expectations and Goals With Your Clinical Mentor
The best mentorships fall apart for one reason: unclear goals and no shared roadmap. Use your first meeting to close that gap before you lose a week of rotation time wondering what you should be learning and how your mentor will know you are making progress.
Map Logistics and Learning Goals Together
Your first conversation should cover two layers. Start with the mechanics: preferred communication method (text, email, or in-person), daily schedule, shift overlap times, and escalation protocol if you encounter a clinical emergency or ethical dilemma and your mentor is off the floor. Then move to learning goals. Do not leave them vague. Instead of saying you want to "get better at time management," specify that you need to chart in real time on a four-patient assignment by the end of week two or that you plan to independently prepare and administer IV medications under supervision by week three. Navigating clinical rotations as a nursing student with this level of specificity from day one makes every shift count.
The Learning Contract: A Simple Tool That Works
Many nursing programs now use a learning contract, a brief document that lists three to six specific clinical skills or competencies you want to develop during the rotation, each with measurable milestones.1 For example: "By week 3, independently manage medication administration for a 3-patient assignment with mentor observation" or "Complete two comprehensive head-to-toe assessments per shift, documenting findings within 30 minutes of completion." The contract should include around nine sections covering objectives, timeline, assessment methods, and sign-off.2 This transforms a fuzzy rotation into a joint project with checkpoints both parties track.
Build Your SMART Goals for the Clinical Floor
Adapt the SMART framework (Specific, Measurable, Achievable, Relevant, Time-bound) to bedside realities.1 A good clinical goal names the skill, the patient load or scenario, the timeframe, and the level of supervision. Poor goal: "Improve critical thinking." Better: "By midpoint review, identify three priority nursing diagnoses for assigned patients within 15 minutes of handoff, validated by mentor." These targets keep daily shifts focused and give your mentor concrete evidence to assess.
Agree on a Communication Cadence
Most rotations benefit from a layered rhythm. Brief daily debriefs of five to ten minutes capture what happened today and set tomorrow's focus.2 One longer check-in each week, lasting 30 to 60 minutes, reviews progress against your learning contract and adjusts goals if needed. Schedule a mid-placement formal review at the 50 percent mark.3 For longer mentorships (capstone, residency, or fellowship), add monthly or bi-monthly sessions to track evolving competencies.4
Use Gibbs Reflective Cycle to Structure Your Debriefs
Post-shift conversations work better with a framework. Gibbs reflective cycle asks six questions in sequence: What happened? What were you thinking and feeling? What was good and bad about the experience? What sense can you make of it? What else could you have done? What will you do next time?5 This structure turns a rambling debrief into actionable learning and ensures your mentor understands not just what you did, but how you are thinking about clinical judgment. Other models (IGROW, CLEAR) also work, but Gibbs remains the most widely adopted in nursing education and fits naturally into a 10-minute wrap-up. Understanding how nurses can avoid common ethics violations becomes far easier when reflective debriefs surface uncomfortable moments in a structured, safe format.
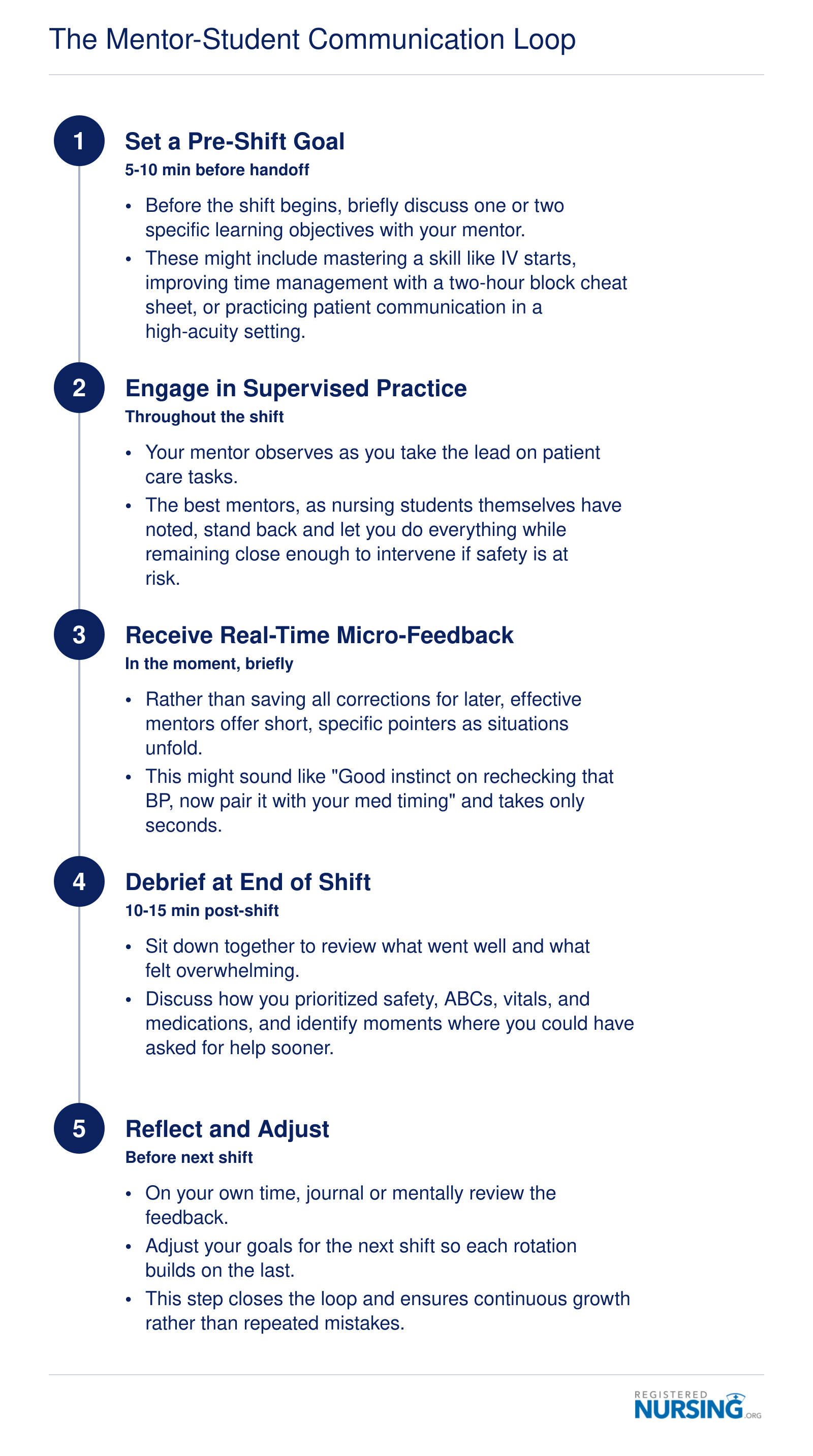
The Mentor-Student Communication Loop
What separates genuine clinical mentorship from passive shadowing is a structured, repeating feedback cycle. When both student and mentor commit to this loop every shift, clinical hours become active learning experiences rather than observation time. The loop below can be repeated across every rotation, whether you are in a BSN, MSN, or DNP program.
Communication Tips: How to Get (And Actually Use) Mentor Feedback
Most students want honest feedback but ask for it in a way that guarantees they won't get anything useful. "How am I doing?" invites a shrug and a "You're doing fine." The tension is between comfort and growth: vague check-ins protect your ego, while specific questions expose gaps you actually need to close. Choose growth, and structure your communication so your mentor can help you.
Ask Precise, Situation-Anchored Questions
Swap the generic check-in for questions tied to a moment your mentor witnessed. Try:
- "Was my assessment of that patient's breath sounds accurate, or did I miss something in the lower lobes?"
- "What would you have done differently during that IV start?"
- "When I called the provider about the potassium, was my SBAR tight enough?"
Specificity gives your mentor something concrete to react to, and it signals that you can handle real answers. Save one or two of these questions for the end of shift when charting is done and there's headroom to talk. This is especially valuable if you're starting nursing school with no clinical experience, since early rotations can feel more like observation than participation.
Receive Critical Feedback Without Flinching
Defensiveness is the fastest way to shut off the feedback pipeline. When a mentor points out something you missed, resist the urge to explain why. A simple "Thank you, can you walk me through the better approach?" does two things: it signals maturity, and it turns criticism into a mini teaching moment. Mentors keep investing in students who use their feedback rather than argue with it.
Advocate for the Level of Involvement You Need
One Reddit commenter, coffeeaddictoops, wished their preceptor had pushed for more independence during a PICU practicum that ended up feeling like regular clinical.1 Another, TheLazyTeacher, described being ditched entirely. Both extremes stall learning. If you're being shadowed too closely, ask directly: "Can I take the lead on medication pass this afternoon and have you observe?" If your mentor disappears, be equally direct: "I need you present for the central line dressing change so you can correct my technique in real time." Balancing work and nursing school adds another layer of pressure, which makes advocating for high-quality clinical time even more important.
Keep a Running Feedback Log
At the end of each shift, jot down what your mentor flagged, what went well, and what you want to work on next time. Patterns emerge quickly across a rotation: maybe your assessments are strong but your time management slips after lunch. That log reveals your real growth areas faster than memory alone, and it gives you a clear starting point for the next shift's conversation.
What Nursing Students Wish Their Clinical Mentors Knew
What do nursing students actually want from their clinical mentors that they rarely say out loud? A recent discussion in the r/newgradnurse community, sparked by a critical care nurse preparing to precept a final semester student, reveals patterns that formal evaluations often miss.1 These candid reflections offer mentors a window into what makes clinical experiences transformative versus merely tolerable.
Graduated Independence Changes Everything
The most consistent theme across student feedback is the desire for progressive autonomy. One commenter described a preceptor who "let them do everything and stood back to watch," calling it a fantastic experience. The contrast came from another student who felt frustrated that their PICU practicum "felt like regular clinical" with no real autonomy granted despite being in a final semester placement.
Students understand they need supervision, but they also recognize that hovering without purpose stunts growth. The sweet spot involves mentors who assess competence early, then deliberately step back while remaining ready to intervene. This graduated release of control builds confidence that carries into the first months of independent practice.
Being Present Is the Baseline
One student offered a blunt wish: they wanted their preceptor to simply not ditch them. While some mentors may step away assuming students need space, disappearing entirely creates anxiety and missed learning opportunities. Presence does not require perfection or constant instruction. It means being accessible when questions arise and available to observe critical moments like medication administration or patient assessments.
Mentors juggling their own patient loads face real constraints, but communicating availability clearly helps. Saying "I need to handle something in room four, but find me if your patient's condition changes" maintains connection without micromanaging.
Practical Workflow Tips Matter More Than Philosophy
The original poster shared concrete advice that students found valuable: using a patient cheat sheet divided into two-hour blocks, labeling items with a permanent marker for quick identification, and learning charting shortcuts in electronic health records. Understanding the advantages and disadvantages of electronic health records can help both mentors and students make the most of these tools during clinical. Gear recommendations included bringing a reliable black pen, badge reel, stethoscope, and trauma shears.
These details might seem minor to experienced nurses who have internalized them, but students operating on cognitive overload benefit enormously from explicit instruction on workflow management. Mentors who share their personal systems for staying organized give students frameworks they can adapt.
Mental Health Acknowledgment Reduces Burnout
The discussion included advice about giving yourself grace, setting a mental "switch off" point during the commute home, and seeking help or therapy when needed.1 Students who see mentors normalize emotional processing learn that sustainable nursing practice includes self-care. Mentors who check in briefly about how students are handling intensity, without prying, create space for honesty about overwhelm. This same awareness of the work environment is worth considering when students reflect on hospital nursing vs. clinical nursing settings and which best suits their temperament.
Clinical mentorship works best when mentors remember what it felt like to be a student: eager to prove competence, anxious about making mistakes, and hungry for someone to believe in their potential.
A great clinical rotation often mirrors the student's own initiative. Those who articulate clear goals, request focused feedback, and immediately put advice into practice routinely extract far more value from the same mentor who might otherwise seem disengaged or distant. Mentorship thrives when you actively cultivate it.
Why Strong Clinical Mentorship Pays Off: Evidence and Career Outlook
Strong clinical mentorship is a documented predictor of nursing success, influencing everything from licensure exam performance to long-term career earnings. The evidence is clear: students who receive quality guidance during clinical rotations graduate with measurable advantages that compound throughout their careers.
Research-Backed Outcomes of Quality Mentorship
Published studies consistently demonstrate that structured mentorship transforms student confidence and competence. According to research in the Asia Pacific Journal of Nursing Research, nursing students in structured mentorship programs saw their clinical confidence jump from 40% to 88% over the course of their mentored experience.1 That near-doubling of confidence translates directly into safer, more effective patient care.
The benefits extend beyond subjective measures. A study of new graduate nurses found that mentorship improved clinical competence scores by 12 to 17 percent, with diagnostic accuracy increasing by 12% and diagnostic errors decreasing by 14%.2 A scoping review of mentorship in nursing and midwifery identified six studies showing skills improvement, six showing job satisfaction gains, five demonstrating better job retention, and four confirming increased confidence.3 These are not marginal effects.
Mentorship as a Career Accelerator
Hospitals with strong nurse mentor programs report retention rate increases of 25%,4 which matters because turnover is expensive and destabilizing. The Be1Support1 mentorship program found that 58.9% of participants said mentorship directly influenced their intent to stay in nursing.5 Meanwhile, meaningful mentorship programs have shown statistically significant reductions in burnout scores among new nurses (P < .01).6
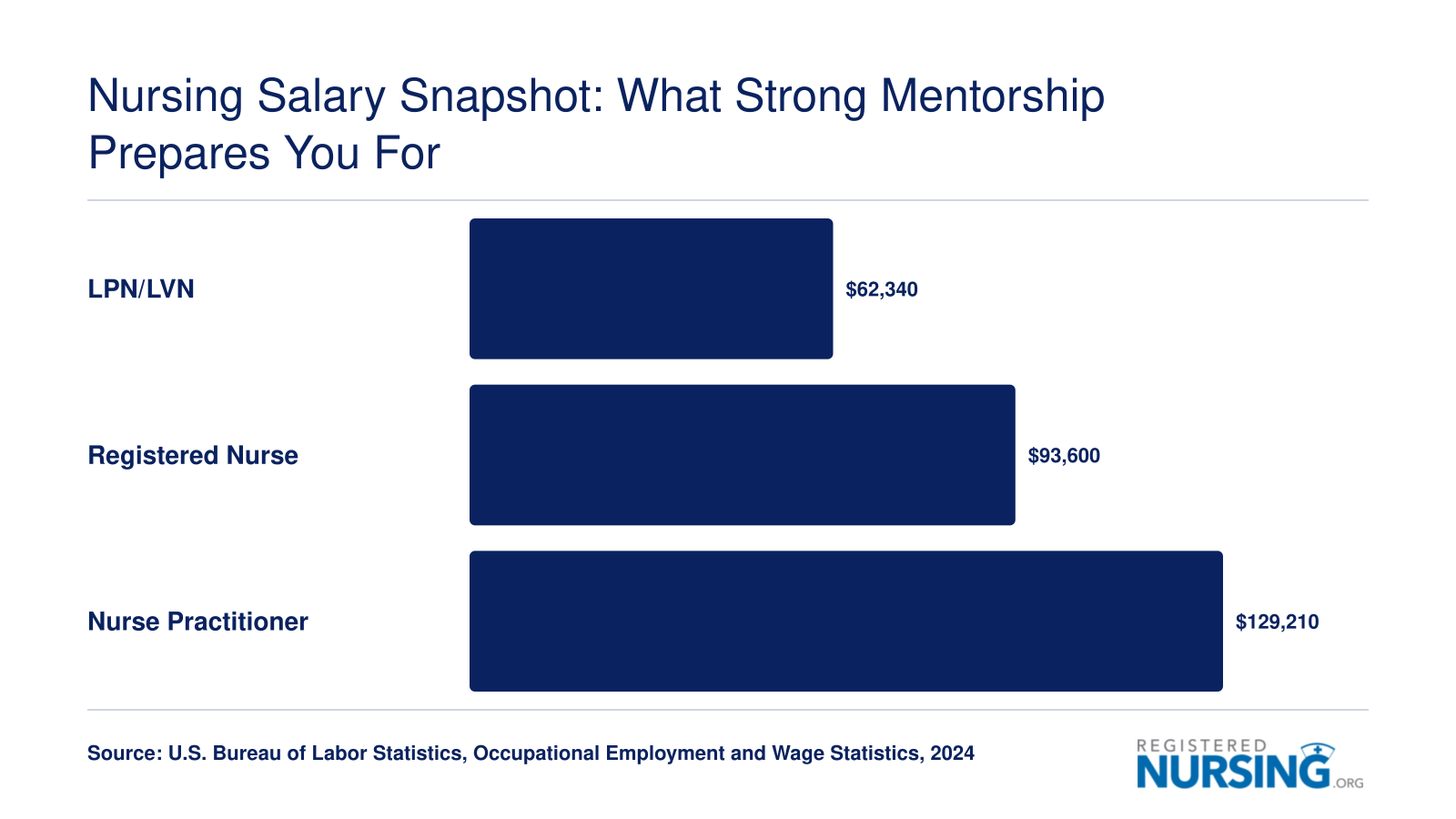
Nurses who feel supported early in their careers are more likely to pursue advanced practice roles. For those considering that path, understanding why a DNP degree is becoming essential can help frame the long-term value of building a strong clinical foundation now. According to current Bureau of Labor Statistics data, registered nurses earn a median annual salary of $93,600, while nurse practitioners earn a median of $129,210. The difference of more than $35,000 per year represents the kind of advancement that strong early mentorship can facilitate.
The Bottom Line for Nursing Students
Mentorship is not a box to check on your clinical rotation form. It is an investment with compounding returns:
- Confidence: Students report more than doubling their clinical confidence through structured mentorship.
- Competence: Diagnostic accuracy and clinical skills improve measurably.
- Retention: Mentored nurses stay in the profession longer and report higher job satisfaction.
- Advancement: Nurses with strong foundations are better positioned to pursue NP, DNP, or specialty certifications. Awareness of barriers to continuing nursing education helps you plan ahead so momentum built in clinical training is not lost later.
When you approach your clinical mentor relationship with intention, you are not just getting through school. You are laying groundwork for a career that could span decades and reach six-figure earnings in advanced practice roles.
Nursing Salary Snapshot: What Strong Mentorship Prepares You For
The clinical mentorship you build during nursing school is your launching pad for every rung on the career ladder. From LPN/LVN roles through advanced practice, each step upward reflects deeper clinical competence, and that competence starts with the skills, confidence, and professional habits your mentors help you develop during rotations.
Frequently Asked Questions About Clinical Mentors in Nursing School
Clinical mentorship can feel unfamiliar the first time you step onto a unit, and it is natural to have questions about how the relationship works. Below are answers to the most common questions nursing students ask about clinical mentors, drawn from the guidance covered throughout this article.
- What is the difference between a clinical mentor and a preceptor in nursing?
- A clinical mentor is a seasoned nurse who offers ongoing professional guidance, career advice, and emotional support across your nursing education. A preceptor, by contrast, is formally assigned to supervise you during a specific clinical rotation, evaluating your competencies and signing off on skills. Mentors focus on long-term growth, while preceptors concentrate on day-to-day clinical performance. Many students benefit from having both.
- How often should nursing students meet with their clinical mentor?
- Frequency depends on your program structure and the mentor's availability, but a good baseline is a brief check-in before and after every clinical shift, plus a longer goal-setting conversation at least once per week. During intensive practicum rotations, daily debriefs help you process new experiences quickly. Even a five-minute conversation about what went well and what felt uncertain can accelerate your learning. The BSN clinical rotation guide offers additional strategies for getting the most from each specialty experience.
- Is clinical mentorship required in BSN, MSN, and DNP programs?
- Most BSN programs build mentorship into senior practicum or capstone courses, where a preceptor works closely with you on the unit. MSN and DNP programs typically require longer mentored clinical hours, often with a faculty-approved preceptor who also functions as a mentor. Formal mentorship policies vary by school, but accreditation standards for advanced-practice programs generally mandate structured, supervised clinical experiences at every level.
- What should I expect from my clinical mentor in a practicum rotation?
- Expect your mentor to prioritize safety, walk you through skills like medication administration and vital-sign interpretation, and gradually foster your independence. As one experienced preceptor in a Reddit discussion noted, the best approach is letting the student do everything while standing close enough to intervene if needed.1 You should also expect honest, constructive feedback and a willingness to answer questions without judgment.
- How do I choose or request a clinical mentor during nursing clinicals?
- Start by talking with your clinical coordinator or program advisor about your learning goals and preferred specialties. Some programs allow students to request a specific unit or hospital, while others assign placements randomly.1 If your program does not offer a formal matching process, reach out to nurses you admire during early rotations and ask if they would be willing to serve as an informal mentor throughout the semester. Nurses who later pursue nurse practitioner school interview questions often credit strong clinical mentors with helping them clarify their specialty focus.
- What are the responsibilities of a clinical mentor in nursing school?
- A clinical mentor is responsible for modeling safe, evidence-based practice, providing real-time feedback, and creating a supportive environment where you can build confidence. Specific duties include guiding you through patient prioritization (safety and ABCs first), helping you develop charting efficiency, encouraging you to ask for help when overwhelmed, and offering perspective on career paths if your current unit does not feel like the right fit.1