What you’ll learn in this article…
- Proactive rapport building turns clinical staff into mentors, not gatekeepers.
- About 63 percent of nursing students report high anxiety during clinicals.
- Treat every clinical shift as a working interview for future job offers.
Nearly two thirds of nursing students experience high state anxiety during clinical training, and most rank clinical rotations as their highest-stress experience during nursing school. A recent Reddit thread captured the raw frustration: a student who felt unwelcome on her unit wondered whether she was failing before she ever touched a patient. That feeling is common and says more about the chaotic reality of understaffed floors than about your potential as a nurse.
Clinicals are where theory collides with real patients, real time pressure, and the personalities of hospital staff. The discomfort is not a sign that you do not belong. It is the price of learning to think and act like a nurse under conditions that are often unfair. Whether you are just beginning to explore entry-level nursing pathways or are already midway through your program, the guidance in this article will help you navigate clinical rotations with more confidence, clearer strategies, and a stronger professional foundation.
What to Expect During Nursing Clinical Rotations
Clinical rotations are where you begin translating classroom theory into real patient care, and knowing what a typical day looks like can ease the uncertainty many students feel before their first shift. While every program and facility operates a little differently, most clinical experiences follow a predictable rhythm and build in complexity as the semester progresses.
The Arc of a Typical Clinical Day
Most clinical days run between 6 and 12 hours and follow a structured pattern:
- Pre-conference: Your clinical instructor gathers the group to review patient assignments, discuss relevant diagnoses, and set learning objectives for the day. You may be asked to present a brief summary of your assigned patient's history and medications.
- Patient assignment and hands-on care: You head to the floor, review the chart, introduce yourself to the patient, and begin assessments, vital signs, medication administration, wound care, or other tasks within your scope. Early in the semester, this often means shadowing a staff nurse; later, you take on more independent responsibility.
- Documentation: You chart your assessments and interventions, either in the facility's electronic health record or on clinical paperwork required by your program. advantages and disadvantages of electronic health records are worth understanding before your first shift, since most facilities use an EHR system.
- Post-conference debrief: The group reconvenes with the instructor to reflect on the day, discuss clinical decisions, and process any challenging moments.
This cycle repeats across each rotation, but the depth of your involvement grows steadily over time.
How Your Patient Load Progresses
Programs ease you in gradually. During your first clinical weeks you may simply observe or assist with basic care under close supervision. By mid-rotation in a med-surg setting, most students manage two to three patients.1 Toward the end of a med-surg rotation, you could be responsible for three to four patients.1 In higher-acuity settings like the ICU, you will typically care for only one patient because the complexity and monitoring demands are far greater.2
By the time you reach a senior practicum or capstone experience, you may carry a near-full patient load alongside a dedicated preceptor, simulating what your first months as a licensed nurse will look like. Preparing for your final clinical rotation well in advance can make that transition noticeably smoother.
How Settings Shape the Experience
Not all clinical sites feel the same, and it helps to know what makes each environment distinct. The BSN clinical rotation guide covers each specialty in detail, but here is a practical overview:
- Med-surg is often the longest rotation (six to ten weeks in many BSN programs) and the fastest-paced for students. You will juggle multiple patients, frequent medication passes, and detailed documentation in the electronic health record.
- Critical care and ICU rotations are typically four to six weeks.2 The pace can feel slower because you have fewer patients, but the acuity is high and the monitoring is continuous. Expect to learn ventilator settings, drip calculations, and hemodynamic parameters.
- Psych and mental health rotations shift the focus from physical tasks to therapeutic communication and behavioral assessment. Documentation tends to be more narrative, and the environment is less procedure-driven.
- Community and public health rotations move you out of the hospital entirely. You may work in schools, clinics, or home health settings, focusing on health promotion, screenings, and population-level data rather than acute bedside care.
Each setting broadens your skill set in ways that are hard to replicate in the classroom.
Understanding the Supervision Chain
Who you report to depends on the clinical model your program uses:
- Instructor-led model: A faculty member accompanies a group of students to the facility. The instructor assigns patients, oversees skills, and must often be present for medication administration. You report directly to this instructor.
- Preceptor model: You are paired one-on-one with an experienced staff nurse (your preceptor) who guides your learning on the unit. Your faculty instructor checks in periodically but is not on the floor full-time. Day-to-day questions go to your preceptor; grading and academic concerns go to your instructor.
- Staff nurse collaboration: Regardless of the model, you will interact with the bedside nurses caring for your assigned patients. Building a respectful working relationship with them is essential, a topic covered in detail later in this guide.
Total Time Commitment
The hours add up quickly. Most ADN programs require roughly 400 to 500 clinical hours before graduation. BSN programs generally mandate 600 to 900 hours, with some programs exceeding 750 hours.4 At the University of Colorado, for example, BSN students complete 765 clinical hours across all rotations.4 Individual rotations vary in length: a single med-surg course might account for about 72 hours,5 while a senior practicum can require 120 to 180 hours on its own.4
Knowing the overall scope of this commitment helps you plan your schedule, arrange childcare or work accommodations, and set realistic expectations for the semesters ahead. If you are balancing a job alongside your studies, working while in nursing school offers practical strategies for managing both.
How to Prepare Before Your First Clinical Day
Walking into your first clinical site unprepared is one of the most avoidable mistakes nursing students make. A little planning the night before can mean the difference between feeling confident and feeling completely overwhelmed.
Start by reviewing the assigned unit or specialty. Look up common conditions, medications, and procedures you are likely to encounter. If you are heading to a medical-surgical floor, for example, refresh your knowledge of wound care, IV medications, and post-operative assessments. The more familiar you are with the clinical context, the easier it will be to absorb what you observe.
Next, confirm the logistics. Know exactly where you are going, how to get there, and where to park. Arriving late to a clinical site sends the wrong message to staff nurses and preceptors before you have even introduced yourself. Lay out your uniform, badge, stethoscope, penlight, and any required paperwork the night before.
Study your program's documentation requirements so you are not scrambling to figure out charting systems on the fly. Many hospitals use electronic health record platforms, and some programs will give you brief orientation materials in advance. Read them.
Think through the soft skills too. Clinicals are as much about professional behavior as they are about technical tasks. Nursing simulation labs can bridge some of that gap before you ever step onto a unit, but real clinical environments demand a different level of readiness. Review your school's clinical handbook, including policies on communication, scope of practice, and incident reporting.
Finally, go in with a learning mindset rather than a performance mindset. You are not expected to know everything. You are expected to be curious, attentive, and respectful. If you tend to feel anxious in social or high-pressure settings, reviewing tips for introverted nursing students ahead of time can help you plan how to introduce yourself, ask questions, and engage with the team without feeling overwhelmed.
Preparation is not about eliminating uncertainty. It is about giving yourself enough of a foundation that the uncertainty feels manageable.
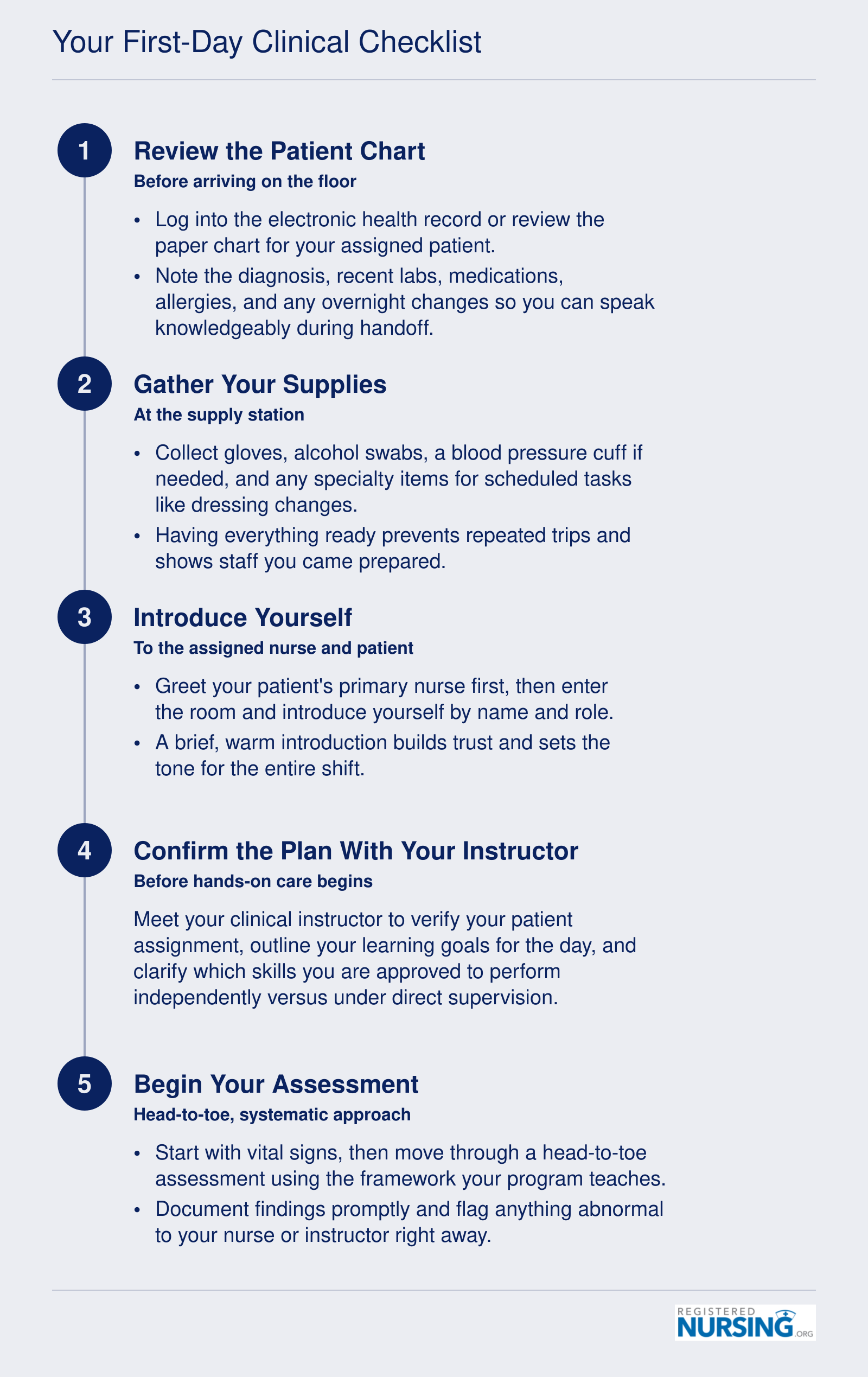
Your First-Day Clinical Checklist
Walking into your first clinical rotation can feel overwhelming, but a clear morning routine keeps you focused and confident. Follow this five-step sequence before you begin any patient care, and make sure your essential gear is packed the night before: stethoscope, penlight, bandage scissors, watch with a second hand, black ink pens, a small notebook, and your school-issued ID badge.
Building Rapport With Nurses and Clinical Staff
Building rapport with nurses and clinical staff means earning their trust and cooperation so they treat you as a contributing member of the team rather than an observer or burden. Strong rapport opens doors to better learning experiences, hands-on opportunities, and professional references that can shape your career.
Why Some Students Feel Unwelcome
Feeling dismissed or unwelcome during clinical rotations is common, and it often reflects the unit's culture, staffing shortages, or stress levels rather than your competence as a student. Nurses working short-staffed or under high acuity may not have bandwidth to orient or teach. Others may have had negative experiences with previous students who required constant redirection or created extra work. Recognize that hostility is rarely personal. Your job is to show up prepared, stay professional, and prove you are there to help, not hinder.
How to Introduce Yourself and Offer Help
Your first impression sets the tone for the entire shift. When you arrive on the unit, find the nurse assigned to your patient and introduce yourself with clear, specific language: "Hi, I'm [your name], a nursing student assigned to [patient name or room number]. I'd love to help. What can I do for you today?" This approach signals competence, respect for their time, and readiness to contribute. Avoid vague offers like "let me know if you need anything." Be explicit about your skill level and what you are allowed to do under supervision.
Trust-Building Behaviors That Make a Difference
Nurses notice students who act like team members rather than spectators. Answer call lights for any patient on the unit, even if they are not assigned to you. Stock supply rooms, replenish linen carts, and help turn or ambulate patients when you see the need. Never stand idle at the nurses' station scrolling your phone. Always close the loop on tasks: if a nurse asks you to check a blood sugar, report the result back promptly and document it. When you finish an assigned task early, circle back and ask what else you can do. These small actions demonstrate initiative, reliability, and situational awareness. For a deeper look at how building trust shapes professional relationships in clinical settings, the principles apply whether you are a student or a seasoned RN.
Handling Dismissive or Hostile Staff
If a nurse is curt, dismissive, or outright rude, stay professional and do not internalize the behavior. Some staff members are not comfortable teaching or simply prefer to work alone. Do not argue, complain to peers within earshot, or disengage. Instead, redirect your energy toward other team members who are more receptive. If behavior crosses a line into harassment, safety concerns, or repeated refusal to allow you to perform required clinical skills, loop in your clinical instructor immediately and document the incidents with dates and details. Persistent hostility that blocks your learning is an instructor problem to solve, not yours to endure silently.
Why Rapport Leads to Better Learning and Career Outcomes
Nurses who trust you teach you more. They let you start IVs, manage complex drips, participate in codes, and take on increasing autonomy. They share clinical reasoning, warn you about unit politics, and model professional behavior under pressure. Many students receive job offers or strong references from nurses they impressed during clinical rotations. The same investment in relationships pays off when you reach your final clinical rotation nursing school capstone, where evaluators weigh your professional presence as heavily as your technical skills. Building rapport is not about being liked. It is about proving you are safe, competent, and worth investing time in. That investment pays dividends throughout your career.
Questions to Ask Yourself
Working Effectively With Your Preceptor and Instructor
How do you work with a preceptor in nursing clinicals without overstepping or underperforming? The answer starts before you touch a single patient.
Set Expectations on Day One
On your first day with a preceptor, ask a direct question: "What would you like me to handle on my own, and what do you want me to check with you on first?" That one conversation prevents the two most common missteps: hanging back when the preceptor expects you to act, or jumping ahead when they expect oversight. Revisit this question each week. As your validated skills grow, your level of independence should shift, but only after your preceptor has seen you perform the skill and agreed you are ready.
The typical progression moves through three stages: observation, assisted practice, and independent practice. If you feel stuck in observation mode after the first few days, it is fair to advocate for more hands-on time. A straightforward way to do this is to say, "I have done this skill in the lab and feel ready to try it with you watching. Would that work today?" That phrasing shows initiative without bypassing supervision. For perspective on what strong preceptorship looks like from the other side, effective preceptor guidance is worth reviewing before your rotation begins.
Know Your Scope Before You Act
Your legal scope of practice as a nursing student is not defined by federal law. It is defined by your state's Nurse Practice Act and your school's approved curriculum.1 What that means practically: a skill you performed at one clinical site may not be permitted at the next, and what is acceptable in one state may be prohibited in another.
State boards are specific about this. Nevada, for example, explicitly prohibits nursing students from performing certain advanced procedures regardless of who is in the room.4 Minnesota permits students to carry out nursing activities taught in the program, but only under instructor supervision.2 Washington ties student scope directly to the RN or LPN scope outlined in state law and to the competencies in the school's curriculum.3
The consistent rule across all states is that you cannot diagnose, order tests, or prescribe medications, and you cannot function as a primary licensed nurse or make independent nursing decisions.1 When you are unsure whether you can perform a new procedure, stop and verify with your instructor. Saying "I need to check with my instructor first" is not a sign of weakness. It is exactly the right response, and experienced nurses will respect it.
Communicate With SBAR
When you need to report a patient concern, use the SBAR framework: Situation, Background, Assessment, and Recommendation. For example: "The patient in room 4 has a new respiratory rate of 24 and is reporting increased chest tightness (Situation/Background); I think his oxygen needs to be reassessed (Assessment); I'd like you to come take a look with me (Recommendation)." That structure signals clinical thinking and makes your communication easy for a busy preceptor to follow. Once you are licensed, working as a registered nurse will demand the same clear, structured communication you are practicing now.
End Each Day With One Good Question
Generic feedback requests get generic answers. Instead of "How did I do today?", close every shift with something specific: "What is one thing I could do differently tomorrow?" That question signals that you are genuinely reflective, gives your preceptor something concrete to offer, and builds the kind of working relationship where honest feedback flows in both directions. Over the course of a rotation, those small daily debriefs compound into real clinical growth.
Mastering Time Management and Patient Prioritization
Time management in nursing clinicals is the practical skill of deciding what to do first, what can wait, and how to keep track of it all when you have multiple patients and a limited shift. It is not about moving faster. It is about moving in the right order, with the right information in hand.
Use the ABCs and Maslow to Decide Who Comes First
When you have two patients competing for your attention, default to the ABCs: Airway, Breathing, Circulation. A patient reporting new shortness of breath outranks a patient asking for pain medication, even if the pain patient rang the call light first. After ABCs are stable, layer in Maslow's hierarchy: physiological needs (oxygen, pain, elimination) come before safety, which comes before comfort and psychosocial needs. A quick example: Patient A needs their scheduled 0900 antihypertensive, and Patient B just returned from the bathroom saying they feel dizzy. Patient B wins. Dizziness could signal a circulation issue, and the med can be given a few minutes later within the administration window.
Group Your Tasks and Build a Realistic Timeline
Cluster care to cut down on trips in and out of rooms. When you enter for 0800 vitals, also do your head-to-toe assessment, hang the scheduled med, check the IV site, and ask about pain and bathroom needs in one visit. A sample two-patient morning might look like: 0700 report and chart review, 0730 brain sheet setup, 0800 Patient 1 full assessment and meds, 0830 Patient 2 full assessment and meds, 0900 chart both assessments, 1000 recheck vitals and any PRN follow-ups, 1030 begin lunch meds prep.
The Brain Sheet Is Your Lifeline
A good nursing worksheet, sometimes called a brain sheet, includes room number, patient initials, diagnosis, code status, allergies, meds due by time, pending labs, IV fluids and site, I&O, and a blank column for notes. Fill it out during report and update it throughout the shift. Understanding how facilities use nursing charting systems will help you adapt your paper notes to whatever EHR platform your clinical site runs.
Avoid the Charting Backlog Trap
The single biggest time drain is trying to reconstruct a shift from memory at 1400. Jot short notes on your brain sheet in real time: vitals, patient statements, PRN times, unusual findings. Chart in short bursts between tasks rather than saving it all for the end.
Protect Your Study Time
Clinicals and coursework will both demand your evenings. Front-load clinical prep (looking up meds, reviewing diagnoses) on the weeknight before clinical, and protect at least one full weekend day for exam study and rest. Trying to do both every night is one of the most common barriers to continuing nursing education that students encounter, and it can lead to burnout by week four.
The students who earn trust fastest are not the ones who know the most, they are the ones who communicate clearly, admit what they do not know, and never try to hide a mistake.
Handling Mistakes, Difficult Situations, and Emotional Challenges
What should you do when you make a mistake during a clinical rotation, and how can you cope with the stress and self-doubt that often follow?
Mistakes, emotional overwhelm, and moments of intense self-doubt are not signs that you chose the wrong profession. They are a predictable part of learning to care for patients in complex, high-stakes environments. What separates students who grow from these experiences from those who get stuck is how they respond.
Responding to Clinical Mistakes
Every nursing student will eventually make an error, whether it is a documentation oversight, a missed assessment finding, or a procedural misstep. The way you handle the moment matters more than the mistake itself.
- Report it immediately: Notify your preceptor or clinical instructor as soon as you recognize something went wrong. Patient safety always comes first, and transparency is a core professional value.
- Resist the urge to hide it: Concealing a mistake can escalate harm and erode trust with the clinical team. Honesty, even when it is uncomfortable, builds credibility.
- Reflect and learn: After the situation is resolved, take time to write down what happened, what led to it, and what you would do differently. Many nursing programs incorporate structured reflection for exactly this purpose.
- Ask for feedback: Use the mistake as a starting point for a conversation with your instructor. You may discover that the error was more common among students than you realized, and your instructor can help you develop strategies to prevent it in the future.
Managing Stress and Anxiety
Clinical rotations can trigger significant anxiety, especially in the early weeks when everything feels unfamiliar. Research in nursing education consistently identifies clinical anxiety as one of the most common challenges students face.
Start by checking your nursing school's website for counseling services, wellness workshops, and academic support centers. Many programs offer targeted resources for managing clinical pressure, including peer mentoring and faculty-led debriefing sessions. If your school provides access to a student wellness program, use it early rather than waiting until stress becomes unmanageable. Developing sustainable habits now is the foundation of self-care for nurses at every career stage.
Organizations such as the American Nurses Association, the National Student Nurses' Association, and the American Psychiatric Nurses Association offer toolkits, free webinars, and fact sheets focused on well-being. These can be practical starting points for learning coping techniques grounded in evidence rather than guesswork. Some of these associations also host member forums where you can connect with other students navigating similar challenges.
Confronting Imposter Syndrome
Feeling like you do not belong on the unit or that you are the only student struggling is remarkably common. This experience, often called imposter syndrome, affects nursing students across all levels of academic performance.
Searching peer-reviewed databases using terms like "nursing student anxiety interventions" or "imposter syndrome in nursing" can help you find evidence-based strategies. Filtering results by recent systematic reviews gives you access to the most current and well-supported recommendations. Even a brief review of this literature can be reassuring, because it makes clear that these feelings are widespread and well-studied.
Practical steps that many students find helpful include:
- Keeping a "wins" journal where you note skills you practiced, questions you answered correctly, and positive feedback from staff
- Talking openly with classmates, because learning that others share your doubts can reduce isolation
- Setting small, specific goals for each clinical day rather than measuring yourself against an unrealistic standard of perfection
Navigating Difficult Interpersonal Situations
Not every nurse or staff member you encounter will be welcoming. Some students experience dismissiveness, being ignored, or even hostility from overworked clinical staff. While this is not acceptable, it is a reality that many students face.
If you encounter a difficult interpersonal dynamic, document specific incidents and bring them to your clinical instructor. Programs take student concerns seriously, and your instructor can intervene, reassign you, or coach you through the situation. Avoid internalizing poor treatment as a reflection of your competence. A staff member's attitude toward students often says more about their workload or workplace culture than it does about you. Understanding the importance of the nurse-patient relationship can also help you refocus on what matters most when the unit environment feels unwelcoming.
The Bureau of Labor Statistics and organizations like the ANA also publish resources on workplace well-being and professional boundaries that can be useful as you learn to manage stress as a nurse throughout your career.
Clinical rotations test you emotionally as much as they test you academically. Building habits around honest self-reflection, early help-seeking, and evidence-based coping now will serve you throughout your entire nursing career.
How Clinical Rotations Are Graded and Evaluated
Understanding how your clinical performance is measured can feel like navigating an opaque system, especially when success depends less on test scores and more on subjective judgment calls about your readiness to care for patients. Unlike classroom exams with clear point values, clinical evaluations assess behavior, decision-making, and professionalism in real time, and many programs use pass/fail or satisfactory/unsatisfactory scales that leave little margin for error. Here's how to decode the rubric, set meaningful goals, and respond to feedback constructively.
Common Rubric Categories
Most ADN and BSN programs evaluate clinical performance across five core domains. Safety and patient harm avoidance is the non-negotiable baseline. Any action that threatens patient safety, such as incorrect medication administration or failure to follow aseptic technique, typically earns an immediate unsatisfactory mark regardless of your performance in other areas.1 Communication includes structured formats like SBAR (Situation-Background-Assessment-Recommendation) handoffs, patient teaching clarity, and teamwork with staff. Professionalism covers punctuality, appearance, respect for confidentiality, and accountability. Critical thinking and clinical judgment assess your ability to recognize changes in patient condition, prioritize interventions, and justify your decisions. Finally, documentation quality measures whether your charting is accurate, timely, and legally defensible.
Some programs use numeric rubrics aligned with the American Nurses Association Standards of Clinical Nursing Practice or QSEN competencies, scoring each domain on a 0-4 scale where 0 represents unsafe practice, 2 signals the need for remediation, 3 indicates competency is met, and 4 reflects exemplary performance.2 A score of 2 or lower in any domain often triggers a remediation plan.
Grading Models: Pass/Fail vs. Letter Grades
Most ADN programs and many BSN programs use pass/fail (or Satisfactory/Unsatisfactory) grading for clinical courses.3 In these models, "unsatisfactory" typically means you demonstrated unsafe practice, failed to meet minimum competency in multiple domains, or showed a pattern of unprofessional behavior. Some BSN programs assign letter grades. For example, one program's rubric translates total scores of 253-272 points into an A, while scores below 181 earn an F.4 In that same program, each unexcused absence deducts 20 points, and any single unsafe act earns a score of zero for the day.
Even when clinical courses are pass/fail, they carry significant weight. You can earn straight As in theory classes but still be dismissed from the program for consistent "needs improvement" marks in clinical. One ADN program explicitly states that a student who fails theory or clinical is withdrawn from the course, and progression requires a minimum C in theory alongside a clinical pass.3
SMART Goals as a Self-Assessment Tool
Many programs require you to write learning goals at the start of each rotation. Effective goals follow the SMART framework: Specific, Measurable, Achievable, Relevant, and Time-bound. A vague goal like "improve my assessment skills" gives you no clear target. A SMART goal looks like this: "By week four of this rotation, I will independently complete a head-to-toe assessment on two patients per clinical day and verbally report abnormal findings to my preceptor using SBAR format within five minutes of discovery." The SMART version tells you exactly what success looks like and when you'll achieve it.
Mid-Rotation and Final Evaluations
Expect a formal evaluation conference midway through your rotation and again at the end. Your instructor or preceptor will review your performance in each rubric category, often using a written form that includes narrative comments. Before the meeting, review your self-assessment, identify one or two areas where you've grown, and prepare a specific question about an area where you want to improve.
If you receive critical feedback, resist the urge to defend or explain. Instead, ask clarifying questions: "Can you give me an example of a situation where I could have communicated more effectively?" or "What specific steps should I take this week to demonstrate improvement in prioritization?" Document the feedback and revisit it weekly. Programs that follow National Council of State Boards of Nursing guidelines must offer a systematic remediation process before dismissal, but that process only works if you act on feedback early.5
Clinical evaluations are not subjective whims. They reflect whether you're developing the judgment, safety habits, and professionalism required to practice independently. Treat each evaluation as data, not a verdict, and use it to refine your approach before the stakes get higher.
Nearly two thirds of nursing students experience high levels of state anxiety during clinical training. A multi-institution study published in a peer-reviewed journal found that 63 percent of students reported significant anxiety while completing their clinical rotations, making it one of the most emotionally demanding aspects of nursing education.
Turning Clinicals Into Career Opportunities
Your Clinical Rotation Is a Working Interview
Every shift you complete is an opportunity to demonstrate your readiness as a future nurse. Many hospitals and health systems hire heavily from their student nurse pools, viewing clinical rotations as extended job interviews. The impression you leave on staff nurses, charge nurses, and managers can directly influence hiring decisions. Treat every interaction as part of your professional brand: arrive on time, stay engaged, and show genuine interest in the unit's work.
Build Relationships With Nurse Managers
Don't wait until graduation to start networking. During each rotation, introduce yourself to the nurse manager or unit director. A brief, professional introduction can open doors: "Hi, I'm [Name], a nursing student completing my preceptorship here. I'm really interested in this unit and would love to learn about new-graduate residency opportunities." Ask about the application timeline and what qualities they seek in new hires. Expressing interest before the rotation ends demonstrates initiative and helps you stand out in a competitive job market.
Secure Meaningful Clinical References
A strong reference from a preceptor or instructor can set your application apart. Ask early, preferably midway through the rotation when your performance is fresh but you still have time to build the relationship. Be specific about what you'd like them to highlight, whether it's your clinical judgment, teamwork, or patient communication. After the rotation, stay in touch with a brief email update on your job search or licensure progress. Maintaining that connection keeps you top of mind when positions open.
Explore Career Paths Through Rotations
Clinical rotations are your chance to explore the many avenues within nursing. A rigorous ICU rotation can be a direct pipeline to a critical care residency, while a psychiatric rotation might reveal a passion for behavioral health. Even if a specialty isn't your first choice, approach it with curiosity: you may uncover an unexpected career path. Some graduates discover entirely new directions, from becoming a travel nurse to pursuing advanced practice roles. Use each rotation to ask nurses about their career journeys and what they love about their field. This exploration helps you make informed decisions about your future.
The Workforce Awaits
According to the most recent Bureau of Labor Statistics data, over 3.3 million registered nurses are employed nationally, with a median annual salary of approximately $93,600. Your clinical performance is the first filter toward joining that workforce. By treating every clinical as a career-building opportunity, you position yourself for a smoother transition from student to professional nurse.
Common Questions About Nursing Clinical Rotations
Clinical rotations raise a lot of questions, especially for students heading into their first placement. Below are answers to the most frequently asked questions, with references to earlier sections of this guide where you can find more detail.
- What are nursing clinical rotations like?
- Clinical rotations place you in real healthcare settings where you care for patients under the supervision of a preceptor or clinical instructor. You will assess patients, administer medications, document care, and practice communication skills. Expect a mix of observation and hands-on tasks that grows more independent as you progress. The earlier section on what to expect during clinical rotations covers the typical structure and daily flow in greater detail.
- What should I bring to my first nursing clinical?
- Essential items include your stethoscope, pen light, bandage scissors, a watch with a second hand, black ink pens, a small notebook, and any required paperwork such as your clinical passport or health clearance forms. Wearing properly fitting scrubs in your program's approved color is also important. If you are starting nursing school with no clinical experience, reviewing a first-day checklist in advance can ease some of the uncertainty. Check the first-day clinical checklist section of this article for a complete, printable list.
- How are nursing students graded during clinical rotations?
- Grading typically combines clinical performance evaluations, written care plans, reflective journals, and professional behavior assessments. Many programs use a pass or fail system, while others assign letter grades. Your preceptor and instructor will evaluate competencies such as critical thinking, patient safety, and communication. The section on how clinical rotations are graded and evaluated breaks down common rubric categories.
- How do you deal with difficult nurses during clinicals?
- Stay professional, introduce yourself clearly, and offer to help with tasks rather than waiting to be asked. If a nurse seems unwelcoming, remember that heavy workloads can affect demeanor. Focus on learning, avoid taking negative attitudes personally, and speak with your clinical instructor if the situation interferes with your education. The section on building rapport with nurses and clinical staff offers practical strategies.
- What happens if you fail a clinical rotation in nursing school?
- Policies vary by program, but failing a clinical rotation usually means you must repeat that course before progressing. Some programs allow one repeat attempt, while others may require a remediation plan or an academic review. A clinical failure does not necessarily end your nursing education, though it can delay graduation. Review the grading and evaluation section of this guide for more context on evaluation standards.
- How do you avoid passing out during clinicals?
- Eat a balanced meal before your shift, stay hydrated, and get adequate sleep the night before. If you feel lightheaded during a procedure, focus on your breathing, slightly bend your knees, and look away briefly if needed. Let your instructor know so you can step out safely. This is more common than students expect, and no one will judge you for it. For broader coping support, the tips in dealing with anxiety as a nervous new nurse can help you build resilience before and during your clinical shifts. The section on handling difficult situations and emotional challenges discusses coping techniques in depth.