
What you’ll learn in this article…
- Research shows NP and physician patient satisfaction scores are nearly equal.
- Longer visit times and communication style drive patients back to NPs.
- Patients still prefer physicians for complex or surgical conditions.
More than 355 million patient visits per year are now handled by nurse practitioners in the United States, yet a persistent question lingers: are patients choosing NPs because they genuinely prefer them, or simply because a physician was unavailable?
The honest answer is that both forces are at work, and separating them matters. Research on patient satisfaction, visit quality, and provider loyalty tells a more nuanced story than either side of the NP-versus-physician debate tends to acknowledge. Condition type, demographics, geography, and state law all shape who patients see and whether they return.
For anyone considering NP practice as a career, that nuance is professionally relevant. The patient preference data does not simply validate NP-delivered care in the abstract; it identifies exactly which care settings, patient populations, and practice conditions produce the strongest outcomes and the highest satisfaction scores. Pediatric nurse practitioner demand offers one clear example of where patient need and provider preference are converging rapidly.
What the Research Says: Do Patients Prefer NPs or Doctors?
Stated preference (who patients say they would choose) versus revealed preference (who they actually see and keep seeing) tells two different stories about provider choice in primary care. Most large-scale research since 2020 focuses on the second: satisfaction after care is delivered.
High Satisfaction Across Both Provider Types
Recent national data shows that patient satisfaction with nurse practitioners reached 75.1 percent in 2026, compared to 67.9 percent for physicians.1 These aggregate numbers, however, mask the more nuanced picture in primary care specifically, where satisfaction rates for all provider types cluster much higher. Studies from 2024 and 2025 report satisfaction scores ranging from 89 to 96 percent for primary care providers broadly, whether NP or MD.2
A 2023 national survey found that 90.3 percent of patients who saw a nurse practitioner expressed willingness to see that same NP again, a strong indicator of trust and continuity.3 A separate 2020 study reported that 81 percent of patients rated their visit satisfaction positively, regardless of provider credential.4 When patients rate specific dimensions of care, NPs consistently score higher on listening skill (80 percent) compared to physicians (50 percent),5 and global satisfaction scores favor NPs at 9.8 out of 10 versus 7.2 out of 10 for physicians.6
Stated Preference vs. Revealed Preference
When asked directly to name their preferred provider type, 55 percent of patients said they prefer a physician, 21 percent said they prefer an NP or PA, and 23 percent reported no preference.7 This stated preference data reflects credential recognition, historical norms, and familiarity more than actual care quality. Many patients do not distinguish between provider types until they experience both. Understanding how physician chart reviews and sign-offs work in states where NP practice is restricted can help clarify how collaborative care shapes the patient experience.
Study Limitations and Context
A 2020 systematic review of ten studies found that four reported higher satisfaction scores for NPs compared to physicians, and none reported lower satisfaction for NPs in comparable primary care settings.8 The remaining studies showed no significant difference.
Nearly all patient preference and satisfaction research published between 2020 and 2026 focuses on primary care and routine outpatient visits. Very few studies examine patient preferences in specialty clinics, urgent care, or surgical contexts, where physician training depth and diagnostic complexity may shift patient perceptions. The current evidence base reflects settings where NP education, scope, and time allocation align closely with patient needs. For NPs considering where to build a practice, the best states for family nurse practitioners vary considerably in scope-of-practice laws, which can directly affect patient access and satisfaction.
Why Patients Choose Nurse Practitioners Over Doctors
Time is the single most powerful currency in healthcare, and nurse practitioners consistently spend more of it with their patients. This difference in visit length, combined with a communication style rooted in nursing philosophy, explains why patients who initially see an NP for convenience often become loyal advocates for NP-led care.
More Time Means Better Care Conversations
The numbers tell a clear story. Nurse practitioners average 34 minutes per appointment compared to 28 minutes for family physicians, a gap of about six minutes that compounds across every question answered, every symptom explored, and every concern addressed.1 Primary care physicians nationally average just 18 minutes per visit, with medians as low as 15.7 minutes,2 yet they typically address six separate topics in that window.3 The math forces trade-offs that patients feel acutely.
In some settings the contrast is even sharper. Canadian NPs in community health centers spend 30 to 60 minutes with patients depending on province,4 while GP consultations in England average just over nine minutes.5 These differences are not accidents of scheduling. They reflect distinct training philosophies and practice models that shape what happens inside the exam room.
Communication Rooted in the Nursing Model
Nurse practitioners are educated in a framework that treats patient education and shared decision-making as core competencies rather than soft skills. The nursing model emphasizes holistic assessment, preventive guidance, and partnership with the patient in setting goals. Where the physician model historically centers on diagnosis and treatment, the NP model begins with the question: what does this person need to understand and feel empowered to do?
This orientation translates into tangible behaviors. NPs are more likely to use teach-back methods, explain medication side effects in plain language, and connect lifestyle recommendations to a patient's actual daily routine. The nurse-patient relationship shapes when a provider sits at eye level, asks about barriers to adherence, and checks understanding before moving on.
Access Opens the Door, Communication Keeps Patients There
Many patients first encounter an NP because of practical factors: shorter wait times for appointments, availability in rural nursing and underserved areas, and lower out-of-pocket costs in some settings. These access advantages get patients through the door. What keeps them coming back is the experience once they arrive.
Surveys consistently show that communication quality, not convenience, is the strongest predictor of provider loyalty. Patients who feel heard and respected during a visit are far more likely to return to that provider, recommend them to family, and follow through on care plans. The NP's training in relationship-centered care turns a first visit driven by scheduling ease into an ongoing therapeutic partnership.
For aspiring nurse practitioners, this pattern offers both validation and responsibility. The clinical strengths that draw patients to NP care are not incidental. They are the direct result of how NPs are taught to practice.
Patients often select a nurse practitioner initially because of shorter wait times or easier scheduling, but they continue seeing that provider because of strong communication and trust. Studies consistently show that the quality of the provider-patient relationship, not credential type, is the most powerful driver of loyalty and long-term satisfaction.
Patient Preference by Care Type: Routine, Chronic, and Complex Conditions
Patient preference for a nurse practitioner versus a physician is not static; it shifts meaningfully depending on the type of care a person needs. Research consistently shows that the complexity of the clinical situation is one of the strongest predictors of whether a patient will choose, or feel comfortable with, an NP as their primary provider.
Routine and Preventive Care: NPs Are Widely Accepted
For wellness exams, immunizations, health screenings, and other preventive visits, patients frequently report no preference between an NP and a physician, and many actively favor NPs. The educational and counseling components of these encounters tend to be where nurse practitioners shine. Because NP training emphasizes patient education and holistic health promotion, patients often feel they receive more thorough lifestyle guidance during routine appointments. Survey data reviewed by the American Association of Nurse Practitioners confirm that satisfaction scores for NP-led preventive care consistently meet or exceed those for physician-led visits.1
Chronic Disease Management: Comparable Satisfaction With a Time Advantage
When it comes to ongoing management of conditions like diabetes, hypertension, and heart failure, patients report high satisfaction with both NPs and physicians.2 NPs may score slightly higher on measures related to time spent with the patient, emotional support, and disease-specific education. These are the very factors that matter most in chronic care, where consistent follow-up and self-management coaching drive outcomes. Continuity of care plays a major role here: patients who see the same NP over multiple visits develop a level of trust and comfort that rivals or surpasses what they report with a physician they see less frequently. For NPs working across hospital and clinic settings, this continuity can be especially meaningful during care transitions.
Acute and Complex Conditions: Physicians Still Preferred
The picture shifts when patients face acute emergencies, rare diagnoses, or conditions requiring complex decision-making or procedural intervention. In these scenarios, patients tend to prefer a physician, citing perceived depth of diagnostic training, direct access to specialist networks, and procedural expertise. Research published in PubMed examining patient preferences found that confidence in a provider's ability to navigate uncommon or high-stakes medical decisions is the primary driver of this preference, not dissatisfaction with NP care in general.3
Familiarity Changes the Equation
One of the most important findings across studies is that experience with an NP recalibrates patient expectations. Patients who have already received chronic disease management from a nurse practitioner report notably higher comfort levels across all care categories compared to patients who have never been treated by one. This familiarity effect suggests that much of the preference for physicians in complex care is rooted in unfamiliarity with NP capabilities rather than in documented differences in outcomes. As NPs continue to expand into more clinical settings and scope-of-practice laws evolve for DNP-prepared nurses, this familiarity gap is likely to narrow further.
Trust, Safety Perceptions, and Diagnostic Confidence
When patients consider switching to or staying with a nurse practitioner, trust sits at the center of that decision. Yet trust is rarely a single judgment. It builds across multiple dimensions: confidence in clinical knowledge, comfort with communication style, and a sense that the provider is genuinely invested in the outcome.
How Trust Forms Between Patients and Providers
Research consistently shows that patients tend to associate trust with how well a provider listens, explains, and follows through. Nurse practitioners, whose graduate training places heavy emphasis on holistic patient education and therapeutic communication, often score well on these relational measures. Many patients report feeling less rushed during NP visits and more comfortable asking follow-up questions, which itself reinforces a sense of confidence in the care they receive.
Physicians, by contrast, are frequently associated with deeper diagnostic authority, particularly for complex or ambiguous presentations. Some patients hold the belief that a physician's longer clinical training translates directly to greater accuracy in diagnosis. Whether or not that perception matches outcomes in every setting, it shapes real behavior: patients with unclear or high-stakes symptoms often seek a physician first. Understanding the difference between an MD, DNP, and Ph.D. in nursing can help clarify how training pathways actually compare.
Diagnostic Confidence and Safety Perceptions
The question of diagnostic accuracy is one of the more nuanced areas in this conversation. Broadly speaking, studies examining patient outcomes across primary care settings have found that NPs deliver care comparable to physicians for a wide range of common and chronic conditions. Differences, when they appear, tend to emerge in highly specialized or complex diagnostic scenarios rather than in routine primary care.
Patient perceptions of safety do not always align neatly with measured outcomes. Some individuals assume that a longer training pathway equals fewer diagnostic errors, which leads them to favor physicians even when an NP is equally qualified to manage their condition. Others, having had a positive and attentive experience with an NP, extend strong trust to that provider's diagnostic judgment as well.
The Role of Continuity in Building Confidence
One of the clearest patterns in the research on trust is that continuity of care matters enormously. Patients who see the same provider repeatedly, whether an NP or a physician, tend to report higher satisfaction, stronger trust, and greater willingness to disclose concerns. For nurse practitioners working in primary care or long-term care settings, this continuity can become a meaningful advantage. A patient who has built a relationship with an NP over months or years is far less likely to question that provider's diagnostic capabilities than a patient meeting any clinician for the first time.
This points to an important insight for aspiring NPs: the foundation of patient trust is laid visit by visit, through attentiveness, accuracy, and follow-through. Credentials open the door; the ongoing relationship is what sustains confidence.
Questions to Ask Yourself
How Demographics Shape Provider Preference
Patient preferences for nurse practitioners versus physicians are not uniform across the population. Research suggests that factors such as age, gender, race and ethnicity, education level, and health literacy all play a role in whether a patient gravitates toward an NP or a physician. However, large-scale, nationally representative surveys that break down preference rates by each demographic group remain limited, and published findings vary across studies and regions.
The Role of Access, Wait Times, and Cost in Patient Choice
Access to care, appointment wait times, and out-of-pocket costs are practical factors that often guide a patient's choice between seeing a nurse practitioner (NP) or a physician. While clinical quality and personal rapport matter, convenience and affordability can tip the scale, especially for routine or non-urgent needs. Understanding these dynamics helps both patients and aspiring NPs appreciate where the profession fits in today's healthcare landscape.
How Wait Times Influence Provider Choice
Long delays for physician appointments are a well-documented pain point in many communities. When patients need care quickly, an NP who can see them sooner becomes an attractive option. Primary care and specialty practices that include NPs often report shorter average wait times for new and returning patients. This benefit is particularly pronounced in underserved areas, where NP-led clinics help fill gaps left by physician shortages.
National workforce data, such as that from the Bureau of Labor Statistics, consistently show strong growth in NP employment, which is tied to increased patient access. While specific benchmarks vary, healthcare systems increasingly rely on NPs to meet demand and keep wait times manageable. For precise numbers on appointment availability, resources like the Medical Group Management Association publish benchmarks that can reveal how NP-inclusive practices compare.
Cost Differences Between NP and Physician Visits
Insurance plan design and billing practices create another layer of patient choice. In many plans, an NP office visit carries a lower copay than a physician visit for the same type of service. This differential can be meaningful for patients with high-deductible plans or those managing chronic conditions that require frequent follow-ups. Retail health clinics and urgent care centers, which are frequently staffed by NPs, often post transparent pricing that appeals to cost-conscious consumers. Nurses at every level can also shape these economics, and ways nurses can influence healthcare organization costs are worth understanding for anyone considering advanced practice.
Public surveys by organizations like the Kaiser Family Foundation track trends in out-of-pocket spending and can illuminate how patients seek value. While data evolves, the general pattern is clear: when patients perceive equivalent quality at a lower direct cost, many will choose the NP. This is not a comment on provider skill but an economic reality of modern healthcare.
The Rise of Telehealth and Retail Clinics
Telehealth has reshaped access in ways that favor NP utilization. Post-2020, many telehealth platforms integrate NPs as primary providers for virtual visits, capitalizing on their availability and patient-centered training. Nurses who want to work in this space often pursue roles as telehealth nurses, where shorter time to appointment and thorough communication are hallmarks of the model. Studies in journals like JMIR document high satisfaction with NP-led virtual care.
Similarly, retail clinics in pharmacies and big-box stores are overwhelmingly NP-driven. The American Association of Nurse Practitioners tracks utilization trends that show growing public comfort with these settings. Patients value the walk-in convenience, extended hours, and predictable pricing, all of which reinforce a preference for NP care in these contexts.
For a deeper dive into the data behind these trends, refer directly to the Bureau of Labor Statistics, Kaiser Family Foundation, AANP, and other authoritative sources. Their reports ground these general observations in verifiable facts, helping you cut through anecdote and understand the measurable factors that steer patient choice.
How Scope-Of-Practice Laws Affect Patient Choice
A nurse practitioner in one state may operate a fully independent primary care practice, while an equally qualified NP in the state next door cannot see a single patient without physician oversight. This patchwork of laws shapes not only how NPs deliver care but whether patients ever get the chance to choose an NP in the first place.
The Three Tiers of NP Practice Authority
As of 2025 and 2026, state laws governing NP practice fall into three broad categories:
- Full practice authority: NPs can evaluate, diagnose, order tests, and manage treatments under the exclusive authority of their state board of nursing, with no mandated physician collaboration.2 Roughly 27 to 30 states and territories, including New York, Washington, Alaska, and Guam, grant this level of independence.
- Reduced practice: NPs must maintain a career-long collaborative agreement with a physician or practice within certain setting-based limits. States like Alabama, Illinois, New Jersey, and Puerto Rico fall into this tier.
- Restricted practice: NPs face career-long requirements for supervision, delegation, or team management by another provider. Large states such as California, Florida, Texas, Georgia, Michigan, and Oklahoma currently operate under restricted frameworks.
These categories are defined by the APRN Consensus Model and tracked through organizations like the American Association of Nurse Practitioners and the National Law Review.
Do Patients in Full-Practice States Choose NPs More Often?
Nationally, surveys show high general acceptance of NPs as primary care providers.3 However, robust state-by-state comparative data on whether patients in full-practice-authority states are measurably more willing to choose an NP over a physician is limited.3 The relationship is difficult to isolate because so many other factors, including provider availability, insurance networks, and local culture, also drive patient decisions.
What we can say is that restricted-practice laws create a structural barrier. In states where NPs cannot practice independently, patients may never encounter an NP as a standalone provider option. That suppresses any measurable preference before it can form. If a patient's insurance panel lists only physician-led practices, the question of "would you choose an NP?" becomes hypothetical rather than practical.
A Clear Trend Toward Expanded Authority
The trajectory is moving toward broader NP independence. The pandemic accelerated this shift, as states temporarily loosened supervision requirements to address provider shortages and then, in many cases, made those changes permanent.4 Legislative activity continues into 2026, with additional states considering bills to grant or expand full practice authority.
For aspiring nurse practitioners, this trend is significant. Practicing in a full-practice-authority state opens the door to independent clinics, direct patient panels, and a clearer path to building the kind of long-term provider relationships that drive patient loyalty. Understanding nurse practitioner vs RN salary differences can also help you weigh the full value of pursuing NP licensure in a state where you can practice to the top of that license. If you are weighing where to practice after graduation, scope-of-practice laws deserve a spot near the top of your decision-making checklist, right alongside cost of living and job availability.
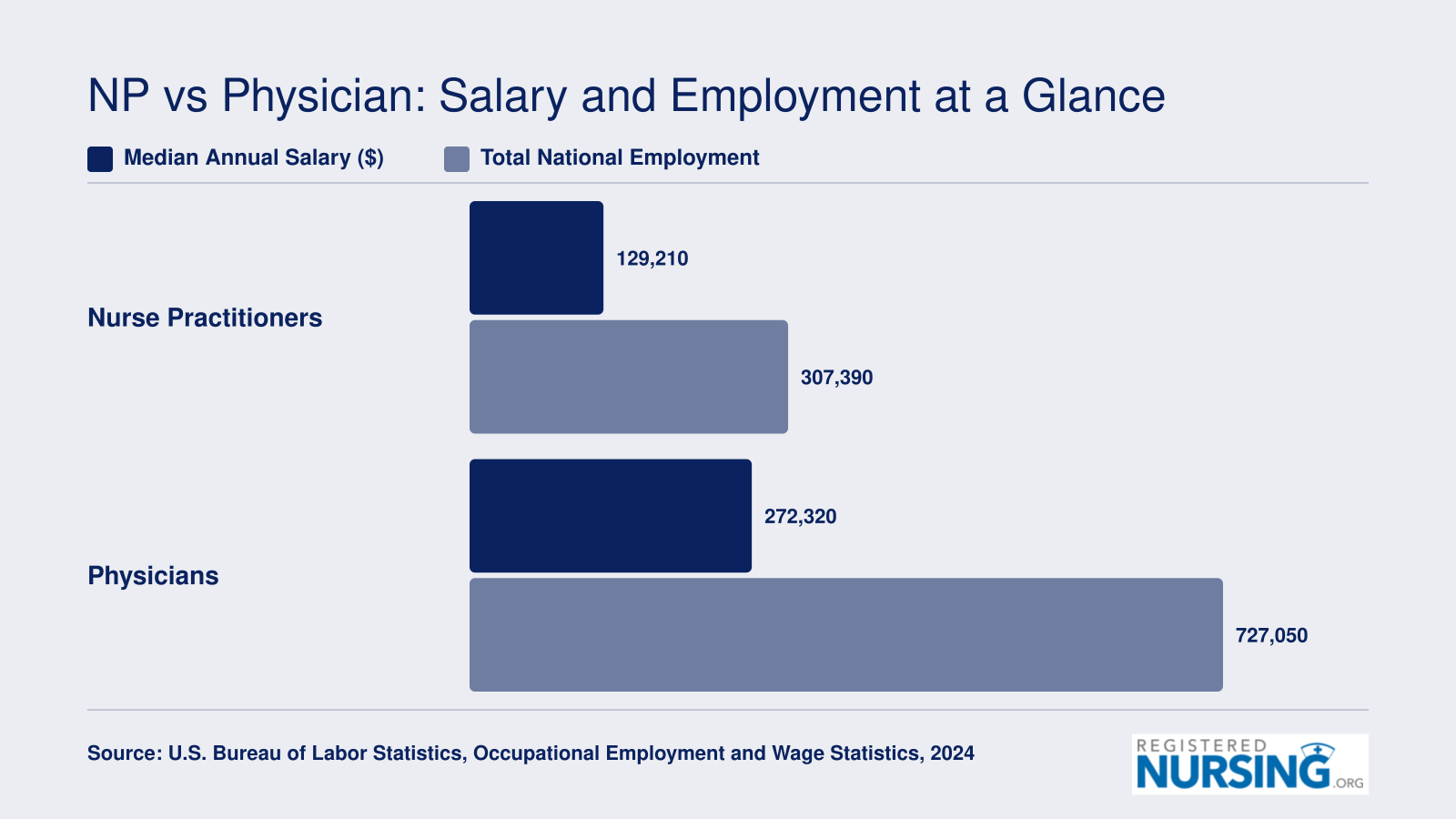
NP vs Physician: Salary and Employment at a Glance
The compensation gap between nurse practitioners and physicians reflects significant differences in training length and scope of practice. However, the rapid growth of NP employment, now exceeding 307,000 nationally, signals that patient demand for NP-delivered care continues to climb. For aspiring nurse practitioners, these figures underscore both a strong earning potential and a profession with expanding opportunity.
What This Means for Aspiring Nurse Practitioners
For anyone weighing the investment of NP school against a longer, more expensive path to physician practice, the patient preference data reframes the tradeoff: what patients say they want most is precisely what NP training is built to deliver.
The Career Value Proposition Lines Up With Patient Demand
Survey after survey points to the same drivers of loyalty: unhurried visits, plain-language explanations, emotional attunement, and a preventive orientation. Those are not soft extras. They are core competencies taught throughout NP curricula, which blend advanced clinical science with the nursing model's emphasis on the whole patient. In other words, the market is asking for the exact provider NP programs are producing. That alignment matters when you are choosing a career that will take two to four years of graduate study and clinical hours. If you are still comparing degree levels early in your planning, which nursing degree to choose can help clarify the path from LPN through BSN before committing to graduate study.
Choosing a Specialization With the Wind at Your Back
Understanding where patient preference is strongest can help you pick a population focus that will stay in demand. A few areas stand out:
- Primary care: Ongoing physician shortages plus patient willingness to see an NP for routine visits make family and adult-gerontology tracks especially durable.
- Chronic disease management: Patients managing diabetes, hypertension, or heart failure consistently rate NP-led coaching and follow-up highly.
- Telehealth and virtual care: Comfort with remote NP visits has grown quickly, opening flexible practice models that did not exist a decade ago.
- Psychiatric mental health: Access gaps are severe, and PMHNPs are moving into roles once reserved for psychiatrists.
A Broadening Scope, a Broadening Career
More states are granting full practice authority, which means new NPs are increasingly able to open independent clinics, lead care teams, and practice without a collaborative physician agreement. The ceiling on autonomy is rising. For those ready to advance even further, affordable online DNP program options offer a practical route to the highest level of clinical preparation. Understanding the difference between an MD, a PA, and an APRN is also useful context as you map out your long-term career position within the broader healthcare team.
As patient satisfaction data continues to accumulate and more people experience NP-led care firsthand, nurse practitioners are moving from a supporting role to a central one in how Americans access healthcare. For prospective students, that is a strong signal about where the profession is headed.
Common Questions About Choosing an NP Over a Doctor
Choosing between a nurse practitioner and a physician is a personal decision shaped by your health needs, preferences, and access to care. Below are answers to the most common questions patients and prospective NPs ask about this choice.
- Is the quality of care from a nurse practitioner the same as from a doctor?
- For primary and routine care, research consistently shows that patient outcomes under NPs are comparable to those under physicians. Multiple systematic reviews have found no significant differences in health outcomes, diagnostic accuracy, or patient safety for common conditions. Physicians typically have more extensive training for complex or rare diagnoses, but for the scope of conditions NPs are trained to manage, the quality of care is on par.
- Do nurse practitioners spend more time with patients than doctors?
- Studies and patient surveys suggest NPs generally do spend more time per visit than physicians, particularly in primary care settings. NP education emphasizes a holistic, patient-centered approach that prioritizes listening, education, and shared decision-making. This extra time often translates into patients feeling more heard and better informed, which is one of the top reasons patients report high satisfaction with NP visits.
- When should you see a doctor instead of a nurse practitioner?
- If you have a complex or rare condition, need surgery, or require care that falls outside an NP's scope of practice, a physician is typically the better choice. Situations involving advanced diagnostics, multi-system diseases, or conditions requiring specialist physician oversight also warrant seeing a doctor. Many NPs work collaboratively with physicians and will refer patients when a case exceeds their training or legal scope. You may also find it helpful to understand whether a DNP can be referred to as a doctor, since the title question often comes up when patients navigate their care team.
- Are patients more satisfied with nurse practitioners or physicians?
- Patient satisfaction scores for NPs are consistently equal to, and in some studies higher than, those for physicians in primary care. Patients frequently cite better communication, more time during appointments, and a stronger sense of partnership as reasons for high NP satisfaction. However, satisfaction can vary based on care setting and condition complexity, with physicians sometimes preferred for specialized or high-acuity care.
- Can a nurse practitioner be your primary care provider?
- Yes. In many states, NPs can serve as your primary care provider with full prescriptive authority and the ability to diagnose, treat, and manage ongoing health needs independently. In states with more restrictive scope of practice laws, NPs may still serve as your primary provider but under a collaborative agreement with a physician. Check your state's regulations to understand how NP practice authority applies where you live.
- Do nurse practitioners prescribe medication the same way doctors do?
- NPs can prescribe medications, including controlled substances, in all 50 states. However, prescriptive authority varies by state. In full practice authority states, NPs prescribe independently. In other states, NPs may need a collaborative agreement or physician oversight to prescribe certain medications. For the majority of routine prescriptions, patients experience no practical difference between receiving a prescription from an NP and receiving one from a physician. Prospective NPs curious about how this and other scope questions are framed during admissions can review common nurse practitioner school interview questions for context.